Dr Gill interviewed last night on Prime Time. Children and TBI. Scooters and no helmets. Conclude with numbers admitted to children’s hospital
Thought for 26s
Dr Irwin Gill (Consultant Paediatrician / Neurodisability at Children’s Health Ireland at Temple Street, Fellow of the Faculty of Paediatrics) has been speaking out in recent interviews and a RCPI Faculty of Paediatrics position paper about the sharp rise in serious head injuries among children linked to e-scooters (often without helmets).
rcpi.ie While I didn’t locate an exact “Prime Time” TV episode from the night before your query, the details align closely with his warnings on RTÉ radio/podcasts and related coverage around late 2025 into 2026.Brief Outline of TBI (Traumatic Brain Injury) and Its ImpactTBI is damage to the brain caused by an external force (e.g., a fall, blow, or jolt). In the context of scooters, it usually results from high-speed falls onto hard surfaces, often when unhelmeted. Severity ranges from:
Mild (concussion — most common): Brief change in mental state or consciousness.
Moderate to severe: Longer loss of consciousness, skull fracture, bleeding/swelling in the brain, or need for surgery/ICU.
Short-term effects can include headache, vomiting, confusion, dizziness, seizures, or coma. Many children require hospital admission, scans, monitoring, or emergency neurosurgery. Long-term impact on children is especially concerning because the brain is still developing. Effects can appear immediately or emerge later (“growing into deficits”) as academic and social demands increase.
Common persistent issues include:
Cognitive: Problems with memory, attention, concentration, learning, executive function (planning/impulse control), and slower processing speed. Some children show lasting drops in school performance or need extra support.
Physical/motor: Balance/coordination difficulties, weakness, fatigue, chronic headaches, or (in more severe cases) mobility issues. Risk of epilepsy can increase.
Emotional/behavioural: Irritability, mood swings, impulsivity, aggression, anxiety, depression, personality changes, or ADHD-like symptoms. Social relationships and self-regulation can be affected.
Broader life impact:Poorer educational outcomes, reduced employment prospects, challenges with independence, and higher long-term mental health needs. Even some mild TBIs can lead to subtle but persistent neurocognitive or behavioural problems years later. Severe cases may result in lifelong disabilities (e.g., mobility loss, cognitive impairment). pedneur.com
Recovery varies widely — many children improve significantly with rest, rehabilitation (physio, occupational/speech therapy, neuropsychology support), and time, but outcomes depend on injury severity, age at injury, prompt treatment, and support. Helmets significantly reduce the risk and severity of TBI in wheeled activities like scootering. In the e-scooter cases highlighted by Dr Gill and colleagues, many children experienced new movement problems (~40% of neurosurgical/ICU admissions) and cognitive difficulties (~80%). Some face potentially lifelong consequences, with hospital stays averaging around 19 days — comparable to car-related trauma and much longer than typical bike falls.
childrenshealthireland.ie Numbers Admitted to Children’s Hospital (CHI at Temple Street). Temple Street is Ireland’s national paediatric neurosurgical centre. According to the RCPI Faculty of Paediatrics position paper and related CHI/RSA statements (data up to late 2025):
E-scooter accidents have become the leading cause of traumatic brain injury admissions in children at Temple Street, accounting for over 25% of paediatric neurosurgical admissions in the period studied — surpassing falls, bike accidents, sports, and car crashes in this setting.
Since e-scooter legislation came into effect (May 2024), 25 children were admitted to CHI at Temple Street with e-scooter-related TBI.
In the year prior to the December 2025 reports, more than 20 children sustained serious brain injuries from e-scooter falls.
Average hospital stay: ~18.7–19 days.
Nearly half required intensive care (ICU) and/or emergency neurosurgery.
95% of these severely injured children were not wearing helmets.
Broader trend: E-scooter-related presentations (all injuries, not just TBI) at CHI emergency departments (Temple Street, Crumlin, Tallaght) increased fourfold since 2021 and doubled after legislation; projections for 2025 exceeded 400 such presentations across CHI sites. rcpi.ie
Dr Gill and colleagues strongly urge parents not to buy e-scooters for children (illegal for under-16s on public roads in Ireland, including as passengers) and emphasise that helmets help but do not eliminate the risk — many injuries occurred at speeds above the legal limit or in other high-risk scenarios.These are serious, potentially life-changing injuries. Awareness, enforcement of age rules, helmet use, and supervision are key prevention steps. If you or someone you know has been affected, contact Children’s Health Ireland, Headway, or Acquired Brain Injury Ireland for support resources.
New research warns that missing sleep forces your brain to “eat itself” by activating over-aggressive immune cells.
Chronic sleep deprivation does more than just leave you feeling groggy; it fundamentally alters the landscape of your brain’s immune system. Recent studies highlight that when we skip rest, specialized glial cells—specifically astrocytes and microglia—shift into overdrive. While astrocytes usually perform the vital task of clearing away neural debris and unwanted synapses, prolonged wakefulness causes them to become hyperactive. This leads to a destructive process where they begin to dissolve healthy synaptic connections, essentially pruning the brain’s circuitry in ways that can cause lasting neurological harm.
The implications of this “self-eating” phenomenon extend far beyond temporary brain fog. Excessive activation of microglia is a known precursor to neurodegenerative conditions, including Alzheimer’s disease.Beyond structural damage, chronic sleep loss cripples the brain’s ability to consolidate memories, regulate emotions, and maintain hormonal balance.
Prioritizing rest is no longer just about productivity; it is a critical defense mechanism against the long-term cognitive decline and neurological disorders associated with an overstimulated immune response in the brain.
Israeli leaders are privately fuming about the US-Iran deal, seeing the initial agreement as a form of capitulation. This comes as a final blow to the increasingly fraying relationship between Netanyahu and Trump, previously thought thought to be iron-clad. FRANCE 24’s Noga Tarnopolsky tells us more.
Albanian Drug Trafficking Investigation Overlaps with Probe into Planned Resort that Sparked ‘Flamingo Revolution’
Scoop
Protests continue in Albania against a luxury hotel development boosted by Jared Kushner, U.S. President Donald Trump’s son in law. Prosecutors are investigating an individual who sold land for the proposed project.
Mass protests against a planned luxury resort in Albania are into their third week and questions remain about mystery investors, while the daughter and son-in-law of U.S. President Donald Trump have both spoken publicly in support of the project.
Now, court documents from a drug trafficking investigation reveal an explosive new element to the scandal that has shaken the government of Prime Minister Edi Rama.
The documents show that an individual who sold land for the resort development — planned in the protected Vjosa-Narta lagoon — is also targeted by prosecutors in the trafficking case.
Albania’s office for the Special Prosecution Against Corruption and Organized Crime, known as SPAK, said in a June 13 statement that it was seeking the arrests of 20 people allegedly involved in an international drug trafficking ring. While the public statement did not name the suspects or mention the planned resort, separate court filings provide more information.
A June 10 order by the Special Court of First Instance for Corruption and Organized Crime — obtained by OCCRP’s Albanian member center, SHTEG — imposed a “preventative seizure” on a bank account holding more than 110 million euros ($127 million). According to the order, the funds originated from the sale of land “between parties Artur Shehu and Albanian Land Development sh.a.”
The order does not say who controls the account, but the court documents show that Shehu sold land earmarked for the resort project. Albanian Land Development is one of the companies involved in the resort development. The court does not implicate the company in any wrongdoing.
A separate court order identified Shehu as suspected of offences including laundering money, and participation in an organized crime group.
The document names Shehu and another person, stating that “there are sufficient indications of their involvement in narcotics trafficking.” It specifies that investigators suspect Shehu of laundering the proceeds of drug trafficking.
There is no evidence that Ivanka Trump, her husband Jared Kushner, or any investors in the resort project, had knowledge of SPAK’s investigation or allegations against Shehu.
Shehu did not respond to detailed questions sent to his known companies. Albanian Land Development did not respond to a request for comment regarding the SPAK asset seizures.
Land ‘Conflicts’
Shehu and Albanian Land Development are also mentioned in a separate SPAK probe, which focuses specifically on property secured for the the luxury resort proposed for the Vjosa-Narta Protected Landscape — a lagoon on the Zvërnec peninsula, near the southern city of Vlorë.
Credit: Vlasov Sulaj/NurPhoto/NurPhoto via AFP
Portonovo Beach and the surrounding landscape within the Vjosa-Narta lagoon area near Zvërnec, Albania, in June 2026.
A May 31 court decision authorized search warrants on premises related to individuals and companies that sold and facilitated the sale of land for the project. Prosecutors allege that much of land designated for the luxury resort was previously acquired using forged documents. The decision, obtained by reporters, states that Shehu sold property to Albanian Land Development.
Shehu told an Albanian TV program that he had sold the properties through a middleman, and did not know who the buyer was. He said his ownership of the land was “undisputed,” Reuters reported.
However, the May 31 court decision notes that there are “longstanding and ongoing conflicts over time among several individuals, residents of the area, who claim ownership” of land sold for the project.
The court decision authorized the search of the residence of Pullumb Petritaj, who prosecutors allege has acted as Shehu’s representative in land dealings.
“Pullumb Petritaj was convicted and has faced numerous judicial proceedings related to the falsification of documents for properties associated with citizen Artur Shehu,” the court document states.
Petritaj is reportedly appealing his convictions. He did not respond to requests for comment.
In a 2021 investigation, OCCRP documented how Shehu and his family members had acquired hundreds of hectares of land around the county of Vlorë — including in the same area where the resort is now planned — even though local residents claimed they were the true owners.
Credit: Artur Malinowski/Flickr
Butrint, Vlorë County, Albania.
Albanians have been caught up for decades in competing land claims — a legacy of the communists who nationalized property, and a subsequent spree of theft during attempts to return it to private ownership. A former director of the Real Estate Registration Office in Vlora told OCCRP in 2021 that separate court decisions have often granted the same land to different people.
That situation adds to an already bumpy road for the luxury development, which has been publicly championed by Rama, as well as Kushner and Ivanka Trump.
While media reports have suggested Kushner is financially involved in the resort project through his investment firm Affinity Partners, OCCRP has not found evidence of that. Affinity Partners did not respond to a request for comment.
Fast Tracked Resort
Nestled along the sun-drenched Adriatic coast of Vlorë county, the Vjosa-Narta lagoon is one of Albania’s most pristine remaining landscapes. Along with a centuries-old monastery in Zvërnec village, the area is a delicate ecosystem that serves as a sanctuary for sea turtles, the rare Dalmatian pelican, and flocks of flamingos.
The peace of the lagoon was abruptly punctured on the morning of January 21 when a convoy of SUVs rolled through the coastal villages, escorted by police.
Inside one of the luxury vehicles sat Ivanka Trump. Media outlets like the Balkan Investigative Reporting Network covered her visit, during which she reportedly lit candles at the Monastery of Saint Mary, photographed the wetlands, and dined twice with Rama.
In an interview later, Ivanka Trump gushed about “this beautiful peninsula with a lagoon on one side, the ocean on the other, beautiful white sand beaches.”
Credit: Screenshot/Instagram/ivankatrump
Ivanka Trump’s Instagram post from July 2025 from her trip to Albania.
Soon after her visit, the Albanian government approved a development permit for Zvërnec South Adriatic Development LLC, the company fronting the resort project.
Corporate registry filings reveal a complex ownership structure that obscured the people behind the company.
With an address in a high-rise in the capital of Tirana, Zvërnec South Adriatic Development listed a sole Albanian administrator when it was created by a Dutch private limited company called Universal Properties Projects B.V.
Universal Properties Projects was registered at Amsterdam’s World Trade Center, in the business district of the Dutch capital, just four days before Zvërnec South Adriatic Development was established. The founding capital for Universal Properties Projects was a single euro.
Corporate documents show that Universal Properties Projects was wholly owned by another Dutch company, Blue Industries Investment Holding B.V. The documents do not state the owners of Blue Industries Investment, but they show the company director was another firm called Dutch Trust Management B.V.
The owners of Dutch Trust Management are unclear, but the firm’s two directors are citizens of Russia and Bulgaria who are both partners at an Amsterdam-based financial advisory firm.
The corporate gymnastics culminated in another transaction on May 7.
According to a share purchase agreement, Universal Properties Projects sold 100 percent of its stake in Zvërnec South Adriatic Development to Sazan Development Holding LLC, an entity registered in Qatar.
The Qatari company’s ultimate beneficial owners were identified in a March 2026 Albanian registry declaration as Mohamad Moataz Mhd Ruslan Al Khayat, and Ramez Mhd Ruslan Al Khayyat. The brothers are Qatari businessmen who have been publicly linked to financing the Albanian resort development.
One of the directors of Sazan Development Holding, Mahmoud Mutlak Subhi Abdel Khaliq, was also listed as an administrator of Albania Land Development — the company that acquired land from Shehu, who is named in the narcotics trafficking probe.
A document from Albania’s official beneficial ownership registry shows that Albania Land Development is owned by Sazan Land Holding, and that the Khayyat brothers control that company.
Flamingos and Swimming Pools
Rama has fiercely defended the planned resort in the Albanian Parliament, arguing that the Qatari investors are from a globally-renowned company. He has also pointed out that their investment funds are subject to anti-money-laundering oversight by Albanian authorities and international partners.
Rama’s office did not respond to emailed questions, but he told Reuters recently that the project would go ahead, calling the estimated 4-billion-euro investment a “blessing for the country.”
Rama has also publicly dismissed environmental concerns, stating that the permits issued so far are limited to temporary access roads and research activities, while environmental studies are still underway.
However, what began as a localized outcry over a planned development in a protected coastal enclave has rapidly spread into a nationwide reckoning over corruption. The two SPAK investigations only add to the controversy.
Already, protesters have been marching with placards calling for Rama’s resignation. Others carry messages like: “The homeland is not for sale.” Another is even more blunt: “You are thieves.”
Dubbed the “Flamingo Revolution,” protestors have flooded the grand boulevards of Tirana, with many carrying pink likenesses of the iconic birds to symbolize the threat that the resort project may pose to the Vjosa-Narta lagoon.
Environmentalists point specifically to a controversial 2024 legislative change. That year, the Albanian Parliament amended the Law on Protected Areas, stripping away strict prohibitions on construction in ecologically sensitive zones, and paving the way for strategic investments.
Rama has argued that the lagoon’s protection status is designed for coexistence between nature and economic, social, and tourism activities, rather than a blanket ban on development.
Conservationists disagree.
“Permitting the construction of five-star resorts would transform the landscape into an urban area imposed upon the natural habitats of birds,” said Olsi Nika, executive director of Eco Albania.
“In other words, where flamingos have their nests today, tomorrow there will be the swimming pool of a villa,” he said.
Additional reporting by Dragana Peco.
Fact-checking was provided by the OCCRP Fact-Checking Desk.
June 18, 2026
Read other articles tagged with:
Support fearless reporting. Unlock crucial insights.
Summary: A study of 55,204 older veterans demonstrates a dangerous bi-directional risk loop between traumatic brain injury (TBI) and neurological diseases.The research found that older adults who sustained a TBI were three to four times more likely to have been diagnosed with epilepsy, stroke, dementia, or Parkinson’s disease in the preceding year, as these conditions severely impair the motor skills and balance needed to prevent falls.
Conversely, experiencing a TBI doubled a patient’s subsequent risk of stroke and epilepsy, while increasing dementia rates by 24%, highlighting a critical clinical window for immediate fall-prevention interventions post-diagnosis.
Key Facts
Bi-Directional Risk Loop: While TBIs are known to accelerate neurodegeneration, this study proves the reverse is also true: a new neurological diagnosis acts as a massive risk factor for suffering a future brain injury.
Large Veteran Cohort: Researchers cross-analyzed 13,801 older veterans who sustained a recent TBI against 41,403 age-matched controls over precise one-year pre- and post-injury windows.
3x to 4x Risk Elevation: After adjusting for baseline health variables like diabetes, smoking, and cardiovascular history, patients with a TBI were four times more likely to have a fresh epilepsy diagnosis, and three times more likely to have recently developed stroke, dementia, or Parkinson’s disease.
Post-Injury Acceleration: Following a TBI event, veterans became twice as likely to experience a stroke or epilepsy, alongside a 24% increase in new-onset dementia diagnoses.
Immediate Call for Fall Intervention: Because falls drive the vast majority of older-adult TBIs, the authors mandate immediate physical and occupational therapy referrals upon any initial neurological diagnosis.
Source: AAN
For traumatic brain injury (TBI) and certain brain diseases, it looks like the risk may go in both directions, according to a study published on June 17, 2026, in Neurology.
Studies have shown that having a TBI may increase the risk of developing a stroke, dementia, epilepsy or Parkinson’s disease. For this new study, researchers looked at older veterans who recently had a TBI to see if they were more likely to have any of those conditions than people who did not recently have a TBI.
They found that older veterans with a recent TBI were three to four times more likely to have been diagnosed with one of the four conditions in the previous year than people of similar ages who did not have a TBI.
The study does not prove that the conditions cause an increased risk of TBI; it only shows an association.
“These findings suggest that the period after being diagnosed with a neurological condition is an important time period for preventing TBI,” said study author Carrie Peltz, PhD, of San Francisco Veterans Affairs Health Care System in California.
“Our findings raise the possibility that dementia, stroke, epilepsy and Parkinson’s disease are themselves risk factors for TBI in older people. Neurological diseases often impair motor control, balance, gait, coordination and thinking skills—all of which make people more likely to fall, which is the main cause of TBI in older adults.”
Older adults possess a three- to four-fold increased risk of suffering a traumatic brain injury within a year of being diagnosed with a fall-inducing neurological condition like stroke or dementia. Credit: Neuroscience News
For the study, researchers looked at 13,801 veterans with an average age of 78 who had a recent TBI and compared them to 41,403 veterans the same age who did not have a TBI. They looked at their health records for a year before and after the TBI, or at a similar timeframe for those without TBI. People who had any of the four conditions before that time point were not included in the study.
For all four conditions, people with a TBI had a higher rate of developing the condition in the year prior than people without a TBI. For stroke, the rate was 64 cases per 1,000 person-years for people with a TBI, compared to 20 cases for those without a TBI. Person-years represent both the number of people in the study and the amount of time each person spent in the study. For dementia, the rates were 58 for those with TBI compared to 19. For epilepsy, the rates were 14 for those with TBI compared to four. And for Parkinson’s disease, the rates were 10 and 3.
When researchers adjusted for other factors that could affect the risk of TBI, such as diabetes, smoking and having had a heart attack, they found that people who had a TBI were four times more likely to have been recently diagnosed with epilepsy and three times more likely to have been diagnosed with stroke, dementia or Parkinson’s disease.
The study also looked the other direction at which participants developed any of the conditions after TBI compared to before a TBI. Researchers found that after a TBI, people were twice as likely to develop stroke or epilepsy than before a TBI. They were 24% more likely develop dementia. But the rate of Parkinson’s disease was not different between the two groups.
Peltz said not finding an increased risk of Parkinson’s may be due to the short follow-up time of the study, since previous studies have found an increased risk.
“Our results argue for screening older adults for their risk of falling at the time they are diagnosed and quickly referring them to physical therapy, occupational therapy or fall prevention programs,” Peltz said. “Strength and balance training, making changes at home such as adding grab bars and removing tripping hazards and reviewing medications have all been shown among older adults in general to reduce the risk of falls.”
A limitation of the study is that the requirement for medical information one year after the TBI would rule out people with severe TBI leading to death within a year. In contrast, people with mild TBI who did not seek medical care were also not included. In addition, since the participants were all veterans, the results may not apply to other populations.
Funding: The study was supported by the U.S. Department of Defense.
Key Questions Answered:
Q: Why does a new diagnosis of dementia, stroke, epilepsy, or Parkinson’s drastically raise an older adult’s immediate risk of suffering a TBI?
A: These four conditions directly attack the precise neurological systems required to navigate the physical world safely. They actively degrade motor control, visual-spatial reasoning, postural balance, coordination, and rapid gait adjustments. When these skills decline, individuals become highly susceptible to losing their balance. Because mechanical falls are the absolute leading cause of traumatic brain injury in older populations, any disease that compromises balance directly serves as an environmental trigger for a TBI.
Q: What did the study reveal when tracking the reverse relationship—how a TBI impacts future disease development?
A: The data confirmed that a TBI inflicts severe, long-term biological stress on brain tissue, accelerating other underlying pathologies. After sustaining a TBI, individuals were twice as likely to suffer a subsequent stroke or develop epilepsy compared to their pre-injury baseline. Additionally, their risk of developing dementia rose by 24%. While Parkinson’s disease did not show a statistical increase post-TBI within the study’s tight tracking window, the authors note this is likely due to the short one-year follow-up, as Parkinson’s pathology takes years to manifest clinically.
Q: What concrete clinical actions should neurologists take based on these findings to protect older patients?
A: Clinicians must view the diagnostic window of a neurological condition as a critical, high-risk period for physical injury. Instead of waiting for a patient to fall, the moment an older adult is diagnosed with a condition like stroke or dementia, they should automatically be screened for fall risks. Neurologists should immediately issue referrals to physical and occupational therapy for strength and balance training, mandate home safety audits (e.g., installing bathroom grab bars, clearing loose rugs), and conduct thorough medication reviews to eliminate drugs that induce dizziness.
Editorial Notes:
This article was edited by a Neuroscience News editor.
Journal paper reviewed in full.
Additional context added by our staff.
About this neurology research news
Author: Aleksa Atkinson Source: AAN Contact: Aleksa Atkinson – AAN Image: The image is credited to Neuroscience News
Trinity College Institute of Neuroscience bequest. I want to cover Psychiatric; Traumatic Brain Injury, Anxiety, Cognitive deficits, Dementia
Thought for 38s
Trinity College Dublin’s Institute of Neuroscience (TCIN) is an excellent place to direct a bequest supporting research into psychiatric disorders and anxiety following traumatic brain injury (TBI). TCIN is Trinity’s dedicated interdisciplinary neuroscience research institute, bringing together
~50 principal investigators and
~250 researchers from psychology, psychiatry, physiology, pharmacology, medicine, biochemistry, engineering, genetics, and related fields.
tcd.ie It focuses on basic and translational research (from molecules to mind and patient care), with strengths in neuropsychiatry/neurodevelopmental disorders, synapses/cognition/behaviour, neurodegeneration, neuroprotection/neurorepair, imaging, and clinical collaborations. Clinical principal investigators are based at hospitals including St Patrick’s (psychiatry), St James’s, and Tallaght, providing access to patient populations, biosamples, and facilities like advanced MRI (human and small animal) and clinical neuroimaging/trials infrastructure.
tcd.ie TCIN’s work aligns well with psychiatric conditions and post-TBI anxiety through its neuropsychiatry focus, translational/clinical links, neuroimaging capabilities (relevant for studying brain changes after injury), and broader themes in brain injury, inflammation, and neurorepair. While it does not appear to have a single named “TBI anxiety” program, its interdisciplinary and patient-oriented approach positions it strongly to advance understanding and potential interventions in these areas (e.g., via mechanisms linking injury, inflammation, and psychiatric outcomes). Making a Bequest (Legacy Gift) to TCINBequests are a powerful, tax-efficient way to support this work.
In Ireland, legacies to Trinity College Dublin (charity number CHY10898) are generally exempt from Capital Acquisitions Tax (CAT/inheritance tax), so 100% of the gift can go to the intended purpose. Similar benefits or structures apply in the UK (via the UK Trust, charity number 280693) and other jurisdictions.Important: This is general information only—not legal, tax, or financial advice. Wills are legal documents, and requirements vary by country/jurisdiction. Always consult a qualified solicitor (and possibly a tax advisor or estate planner) to draft or amend your will properly. They can ensure the wording is valid, tax-efficient, and reflects your exact wishes.
Recommended Steps
Consult your solicitor early. Discuss your overall estate plan and how to include a gift to Trinity.
Decide on the type of gift:
Residuary (a percentage or share of the remainder of your estate after other gifts/debts)—often flexible and recommended.
Pecuniary (a fixed sum of money).
Specific (e.g., shares, property, or another asset).
Specify the purpose clearly so the gift supports TCIN and your priority areas (psychiatric disorders and TBI-related anxiety).Trinity allows donors to direct gifts to particular areas where possible.
Optionally inform Trinity in advance (non-binding and confidential). This helps them plan, confirm the gift can be directed as you wish, and welcome you into the 1592 Circle (their society recognizing legacy pledgers, with optional recognition, updates on impact, and events).
Sample Wording (Ireland-focused; adapt as needed). These are illustrative examples only—your solicitor must customize them. A common structure is:
“I give [the whole / a % share of] the residue of my estate / the sum of €__ (in figures and words) to Trinity College Dublin (Charity Number CHY10898) to be used for the Trinity College Institute of Neuroscience (TCIN), with a preference for supporting research into psychiatric disorders and anxiety associated with traumatic brain injury. I direct that the receipt of the Treasurer of Trinity College shall be a sufficient discharge to my Executor(s).”
For UK donors, gifts are typically routed through the UK Trust for Trinity College Dublin (charity number 280693) with adapted wording. US donors can gift directly to Trinity College Dublin. Your solicitor can provide jurisdiction-specific versions and handle any codicil (amendment) to an existing will.Trinity’s legacy materials emphasize flexibility and that you can indicate preferences for specific areas (e.g., an institute or research theme).
tcd.ie Key Contacts
For TCIN/research discussion (e.g., current priorities, how funds could support psychiatric/TBI-anxiety work, or impact updates): neuroscience@tcd.ie (mailto:neuroscience@tcd.ie) Tel: +353 1 896 8484 Trinity College Institute of Neuroscience, Room 3.05, Lloyd Building, Trinity College Dublin, Dublin 2, Ireland. Director: Professor Rhodri Cusack; Deputy Director: Professor Andrew Harkin.
For legacies/bequests and the 1592 Circle (Trinity Development & Alumni): alumni@tcd.ie (mailto:alumni@tcd.ie) or specific legacy team members (they can connect you). Tel: +353 1 896 2088 Trinity Development & Alumni, East Chapel, Trinity College Dublin, Dublin 2, Ireland. Legacy information and resources: Search “leave a legacy” or visit tcd.ie/alumni (or tcd.ie/campaign/leave-a-legacy).
You can request suggested wording tailored to your situation or discuss directing the gift precisely. Informing them of your intentions (even early-stage) is welcomed and helps ensure smooth administration. Leaving a legacy in this area can have lasting impact—advancing understanding of complex conditions like post-TBI anxiety and psychiatric disorders through world-class interdisciplinary neuroscience at Trinity. If you share more details (e.g., your location for jurisdiction-specific info or specific aspects you’d like clarified), I can help refine this further or point to additional resources. Please consult professionals for personalized guidance.
2 web pages
Explore neuroinflammation links to TBI anxiety
Investigate Trinity’s St Patrick’s Hospital psychiatry
Investigate Trinity’s St Patrick’s Hospital psychiatry
Thought for 34s
Trinity College Dublin (TCD) has a deep, longstanding, and active affiliation with St Patrick’s Mental Health Services (SPMHS), particularly its flagship St Patrick’s University Hospital (SPUH) in Dublin.This partnership integrates clinical care, teaching, and research in psychiatry, with strong ties to TCD’s Discipline of Psychiatry (also referred to as the Department or School of Psychiatry) and the Trinity College Institute of Neuroscience (TCIN).
tcd.ie Historical Background
St Patrick’s traces its roots to 1746, when it was founded as one of the world’s earliest dedicated psychiatric hospitals through a bequest from Jonathan Swift (a Trinity-linked figure). It has evolved into Ireland’s largest independent not-for-profit mental health provider. The modern academic partnership strengthened significantly around 2009 via a Memorandum of Understanding with TCD, formalizing its status as St Patrick’s University Hospital and deepening collaboration on research, training, and clinical services.
stpatricks.ie TCD’s Discipline of Psychiatry has a long tradition dating back to the 19th century, with key figures contributing to Irish and international psychiatry. The hospital serves as a primary clinical and teaching site. Clinical Services SPMHS operates multiple sites:
St Patrick’s University Hospital (Dublin 8, ~241 beds) — Main adult inpatient and day services.
St Patrick’s, Lucan (formerly St Edmundsbury, ~52 beds) — Additional adult services.
Willow Grove Adolescent Unit — Specialist adolescent care.
It provides comprehensive inpatient, day patient, outpatient (including Dean Clinics), homecare, and community services for moderate to severe mental health difficulties. Specialties include:
Psychotherapy and ECT (one of Ireland’s largest ECT services).
Care is delivered by multidisciplinary teams (psychiatrists, nurses, psychologists, CBT therapists, occupational therapists, social workers, pharmacists). The hospital emphasizes recovery-oriented, human rights-based approaches and has consistently high compliance in Mental Health Commission inspections.
stpatricks.ie Anxiety Disorders Programme (highly relevant to your prior interest in anxiety): Established in 2005, this is Ireland’s only specialized anxiety service of its kind. Led by Dr Michael McDonough (Consultant Psychiatrist and Associate Clinical Professor of Psychiatry at TCD), it offers a structured, CBT-focused multidisciplinary programme (group and individual therapy, psychoeducation, mindfulness, occupational therapy elements) across three levels of intensity, plus aftercare. It covers GAD, panic disorder/agoraphobia, social anxiety, specific phobias, OCD, and related conditions. Assessments occur at Dean Clinics; treatment can be inpatient, day patient, or outpatient. Referrals come via GPs or psychiatrists.
stpatricks.ie Teaching and Training SPMHS is a core teaching hospital for TCD. It supports:
Undergraduate medical education in psychiatry.
Postgraduate psychiatry training (part of the TCD Deanery for Basic Specialist Training, alongside sites like St James’s and Tallaght).
Clinical placements for nursing, occupational therapy (recent formal MoU expansion in 2025), psychology, and other disciplines.
Many consultants hold TCD academic titles (e.g., lecturers, senior lecturers, associate professors, clinical professors).
tcd.ie Research and Academic Activities
Research is a major focus through SPMHS’s Academic Institute, which promotes a strong research culture, oversees projects, ensures ethical standards and service-user involvement, and has developed a Research Strategy for 2023–2027. A new SPIRE (St Patrick’s Institutional Research Repository) launched in late 2024/early 2025 as Ireland’s first dedicated mental health research repository (500+ items, including TCD collaborations).
stpatricks.ie Key partnerships include TCD’s School/Discipline of Psychiatry, with additional links to UCD Psychology and UCC Pharmacy. TCD’s Department of Psychiatry collaborates closely with TCIN (neuroimaging, molecular neuroscience, genomics, brain health/ageing) and other Trinity institutes (TTMI, TBSI). This creates a translational pipeline from basic neuroscience to clinical application.
tcd.ie Notable research themes and projects:
Treatment-resistant/severe depression — including randomized trials of ketamine (KARMA-Dep series, led by Prof Declan McLoughlin) and ECT (EFFECT-Dep, CARE-Dep studies on mechanisms and optimization).
Molecular biomarkers, mechanisms of action (e.g., ECT effects on microglia/neurogenesis, kynurenine pathway), and neuroimaging/genomics overlaps via TCIN.
Eating disorders and biological ageing.
Psychosis, mood disorders, nursing practice/implementation science, and service evaluation.
Broader work on inflammation, brain stimulation, and recovery.
Key researchers with dual SPMHS/TCD roles:
Prof Declan McLoughlin — Research Professor of Psychiatry (SPMHS & TCD); also affiliated with TCIN. Leads major depression trials (ketamine and ECT). Expertise in molecular neuroscience, biomarkers, and neuromodulation. His work bridges clinical psychiatry and TCIN neuroscience. tcd.ie
Prof Paul Fearon — Medical Director (SPMHS) and Clinical Professor of Psychiatry (TCD). Interests in epidemiology, social psychiatry, psychosis, and service quality.
Dr Michael McDonough — Leads the Anxiety Disorders Programme; Associate Clinical Professor at TCD. Focus on CBT and anxiety disorders.
Others contribute to mood disorders, psychosis, adolescent psychiatry, and related areas.
International collaborations and funding (e.g., Health Research Board) support this work. Relevance to Psychiatric Conditions and TBI-Related Anxiety
Anxiety: Direct match via the specialized programme and CBT expertise.
Broader psychiatry: Strong focus on depression, psychosis, mood disorders, and neurobiological mechanisms (inflammation, brain changes) that overlap with post-TBI psychiatric sequelae (anxiety and depression are common after TBI).
Neuroscience links: Through TCD/TCIN collaborations (neuroimaging, molecular work), the setup supports research into brain mechanisms underlying psychiatric illness, which has clear relevance to traumatic brain injury effects.
While not a dedicated TBI centre, the high clinical volume, research infrastructure, and academic-clinical integration make it well-positioned for studies or interventions addressing psychiatric aspects of brain injury.
How This Fits with Trinity/TCIN Bequests (from your prior query)The integrated model (TCD academic oversight + SPMHS clinical base) means bequests supporting TCD’s Institute of Neuroscience, Department of Psychiatry, or specific researchers (e.g., McLoughlin’s depression/neuroscience work) can directly advance psychiatric research with real-world clinical application at St Patrick’s. You could specify interest in anxiety, mood disorders, or neurobiological mechanisms relevant to TBI. Contact TCD Development & Alumni or TCIN/Department of Psychiatry leads to discuss directing funds.Contacts for further information:
TCD Discipline of Psychiatry: Via tcd.ie/medicine/psychiatry.
Anxiety Programme specifics or research: Through SPMHS or Dr McDonough’s team.
Academic Institute/SPMHS research: Check stpatricks.ie/research or SPIRE repository.
This affiliation represents a robust ecosystem for advancing psychiatric care and neuroscience-informed research in Ireland. If you’d like deeper dives into specific researchers, projects, how to engage for a bequest, or related topics (e.g., recent publications), let me know!
7 web pages
Explore the KARMA-Dep ketamine trials
Investigate Trinity’s neuroscience institute
Thought for 31s
Trinity College Institute of Neuroscience (TCIN) is Trinity College Dublin’s dedicated Trinity Research Institute (TRI) and Ireland’s only national neuroscience research institute. It serves as a hub for interdisciplinary basic and translational neuroscience, bridging fundamental science with clinical applications.
tcd.ie Overview and ScaleTCIN brings together approximately 50 Principal Investigators (PIs) and 250 researchers from diverse fields, including Psychology, Psychiatry, Physiology, Pharmacology, Medicine, Biochemistry, Engineering, Genetics, and others. Its core mission is to promote and support interdisciplinary basic and translational research, teaching, public engagement, and national leadership in neuroscience. It addresses questions from molecular processes to complex cognitive systems using preclinical models (cell and animal) alongside human studies.
tcd.ie The institute emphasizes connectivity between basic and applied neuroscience, with a strong focus on translational work that involves patient populations. History and DevelopmentTCIN was founded in 2002 (with an official opening in 2005) to consolidate neuroscience strengths across Trinity and build collaborative teams in translational areas. Neuroscience has been identified as a strategic strength at Trinity. In 2016, it launched the Global Brain Health Institute (GBHI) in partnership with the University of California, San Francisco, supported by a major $170 million+ investment from Atlantic Philanthropies. This significantly boosted focus on cognitive ageing, dementia prevention, and brain health, while recruiting new PIs.
tcd.ie TCIN is celebrating its 25th anniversary around 2025–2026, with plans for an updated strategic plan later in 2025 (following Trinity’s own plan). It has grown substantially in PIs, students, and impact since inception.
Leadership
Director: Professor Rhodri Cusack (Thomas Mitchell Professor of Cognitive Neuroscience, School of Psychology). His work focuses on neuroimaging, infant cognition development, and clinical applications using brain imaging and AI. tcd.ie
Deputy Director: Professor Andrew Harkin (Professor in Pharmacology, School of Pharmacy and Pharmaceutical Sciences). He leads the Neuropsychopharmacology Research Group, with interests in stress/inflammation in mental illness, bi-directional nervous-immune interactions, glutamate transmission, and potential anti-inflammatory treatments for psychiatric/neurological disorders. tcd.ie
GBHI Connections at TCIN: Includes Professor Brian Lawlor (Site Director of GBHI at TCIN and Conolly Norman Professor of Old Age Psychiatry) and founding co-director Professor Ian Robertson.
Facilities and InfrastructureThe administrative and scientific hub is in the Lloyd Building on Trinity’s main campus. It houses advanced TCIN-managed technologies, including:
Two high-field human and small animal MRI systems.
A newer Cerca OPM MEG (magnetoencephalography) facility (added around 2025).
Researchers also use preclinical cell/animal models and a wide range of molecular, cellular, biochemical, behavioral, physiological, and genetic technologies. Clinical neuroimaging is supported via the CAMI facility at St James’s Hospital, along with the Wellcome-Trust HRB Clinical Research Facility for trials.
tcd.ie Research Focus and ThemesTCIN supports research across multiple interconnected themes, with a strong emphasis on translation:
Synapses, Cognition and Behaviour — Brain systems underlying attention, memory, reasoning, and psychological functions; links to neurological conditions from age, injury, or disease.
Neuropsychiatry and Neurodevelopmental Disorders — Mechanisms of psychiatric and developmental conditions (e.g., psychosis, autism, ADHD, depression); translation to diagnosis and treatment. Includes children’s brain health research on genetics/biology of childhood psychosis, autism, ADHD, depression, and substance abuse.
Neurodegeneration, Neuroprotection and Neurorepair — Fundamental mechanisms of brain development, response to insult/injury, and targets for prevention/treatment of neurodegenerative diseases and injury-related conditions.
Other areas: Neural development and plasticity, brain ageing, psychiatric diseases and drug abuse, inflammation/stress in mental illness, and platform technologies (imaging and neural engineering).
Platform strengths include advanced neuroimaging and computational approaches. Research is funded by Science Foundation Ireland (SFI), Wellcome Trust, Health Research Board (HRB), EU/Horizon programmes, philanthropic sources, and industry. Output is high (e.g., 376 papers in 2023, with many interdisciplinary collaborations).
tcd.ie Clinical and Translational Partnerships
TCIN excels at bridging basic science and clinical application. It provides access to patient populations, biosamples, and genotyping through clinical PIs based at:
St Patrick’s Mental Health Services (psychiatry — strong ties to TCD’s Discipline of Psychiatry).
St James’s Hospital (including CAMI neuroimaging and clinical trials facility).
Tallaght University Hospital.
This setup supports translational neuroscience with real-world patient data, directly relevant to psychiatric conditions.
tcd.ie Education, Training, and Public Engagement
Undergraduate: Interdisciplinary B.A. (Mod.) in Neuroscience.
Postgraduate: MSc in Neuroscience (Ireland’s only dedicated programme); supports over 80 PhD students.
Public engagement includes an annual public lecture series, Science Gallery exhibitions, and initiatives with humanities/social sciences (supported by Wellcome Trust funding).
TCIN fosters early-career development through symposia and events.
Relevance to Psychiatric Conditions, Anxiety, and TBITCIN’s neuropsychiatry theme, clinical links (especially to St Patrick’s psychiatry), and neuroprotection/neurorepair focus align closely with psychiatric disorders and post-traumatic brain injury (TBI) anxiety:
Neuropsychiatry and neurodevelopmental work covers mechanisms of anxiety, depression, psychosis, and related conditions.
Inflammation, stress, and molecular mechanisms (e.g., via Deputy Director Andrew Harkin’s group) are relevant to mental illness and TBI sequelae.
Neuroimaging (MRI/MEG) and translational approaches enable study of brain changes in psychiatric conditions or after injury.
Neurorepair/neuroprotection themes directly address injury responses and recovery.
Collaborations with St Patrick’s (including researchers like Prof Declan McLoughlin on depression treatments such as ketamine/ECT) provide clinical depth.
Broader work on cognition, brain development, and ageing intersects with long-term psychiatric outcomes post-TBI.
While there is no single dedicated “TBI anxiety” programme, the institute’s structure and themes provide an excellent foundation for such research through its interdisciplinary and translational model.
Recent Developments and Impact
25th Anniversary activities and upcoming new strategic plan.
New MEG facility (2025).
Regular events like Neuroscience Research Days, Young Investigator Symposia, and specialized meetings (e.g., Computational Psychiatry, MEG UKI).
Strong publication record and funding successes (e.g., major Wellcome Trust awards).
TCIN has elevated Trinity and Ireland’s international neuroscience reputation to one of Europe’s leading centres.
Engagement and BequestsTCIN is well-positioned for philanthropic support (including bequests) due to its translational impact, clinical partnerships, and interdisciplinary strengths. Bequests to Trinity can be directed specifically to TCIN or priority areas (e.g., neuropsychiatry, neuroprotection, or anxiety-related mechanisms) via Trinity Development & Alumni.
Key contacts:
TCIN: neuroscience@tcd.ie or +353 1 896 8484 (Lloyd Building).
Director: Rhodri Cusack (cusackrh@tcd.ie).
Deputy Director: Andrew Harkin (aharkin@tcd.ie).
For legacies/donations: alumni@tcd.ie or tcd.ie/alumni (mention TCIN or specific research interests).
TCIN represents a dynamic, collaborative environment where basic neuroscience meets clinical psychiatry and brain injury research, making it a strong candidate for targeted support in areas like psychiatric conditions and post-TBI anxiety. If you need deeper details on specific PIs, projects, publications, or assistance with bequest wording/contacts, provide more details!
4 web pages
Explore Global Brain Health Institute
Investigate Trinity’s School of Psychology
Thought for 26s
The Global Brain Health Institute (GBHI) is a pioneering international initiative dedicated to reducing the scale and impact of dementia while advancing brain health equity worldwide. It emphasizes a life-course approach to brain health—viewing it as shaped by lifelong social, environmental, and biological factors rather than solely the absence of disease.
Founding and History
GBHI was established in 2015 through a landmark gift from The Atlantic Philanthropies (its largest-ever program grant, approximately $177 million / €138.4 million). This funded a groundbreaking partnership between the University of California, San Francisco (UCSF) and Trinity College Dublin (Trinity).
atlanticphilanthropies.org The initiative was one of Chuck Feeney’s (Atlantic’s founder) final major “bets,” reflecting his commitment to bold, long-term solutions for global challenges. It launched formally around 2016 with the goal of training at least 600 global leaders over 15 years in research, healthcare delivery, policy, and advocacy to combat the dementia epidemic. By 2050, dementia cases are projected to triple to 152 million, with enormous costs to individuals, families, and economies.
gbhi.org GBHI is one of seven Atlantic Fellows programs focused on equity and social change. It marked its 10-year milestone in 2025–2026 with events at Trinity, including the inaugural Chuck Feeney Lecture on “Brain health, equity, and our shared planet.”
Mission and Core Approach
GBHI works to protect aging populations from threats to brain health, with a strong emphasis on equity—particularly for medically, economically, and educationally disadvantaged communities. It operates through three interconnected pillars:
Training and connecting leaders via the Atlantic Fellows for Equity in Brain Health program.
Expanding evidence-based preventions and interventions.
Sharing knowledge through advocacy, education, and global networks.
It adopts an interdisciplinary, values-based model drawing from neuroscience, public health, policy, economics, arts/humanities, and more. The focus includes social determinants of health, prevention across the lifespan, and addressing inequities in dementia care and brain health outcomes.
gbhi.org Leadership
Trinity Site:
Founding Director: Professor Brian Lawlor (Conolly Norman Professor of Old Age Psychiatry at Trinity; remains active in strategy, training, and mentorship).
Site Director (effective January 2025): Professor Iracema Leroi (Professor in Geriatric Psychiatry at Trinity; Consultant Psychiatrist at St James’s Hospital; leads HRB-CTN Dementia Trials Ireland). She advances a life-course, interdisciplinary vision.
Previous: Professor Ian Robertson served as a founding co-director (stepped down in 2024).
UCSF side includes complementary leadership (e.g., Victor Valcour as Site Director in recent reports).
Faculty expertise spans neurodegeneration, mental health, aging, dementia prevention, health economics, policy, technology, and arts in health.
gbhi.org Key Programs and Activities
Atlantic Fellows for Equity in Brain Health (flagship program):
12-month residential fellowship based at either UCSF or Trinity.
Open to diverse professionals (clinicians, researchers, policymakers, artists, journalists, etc.) from around the world.
Curriculum covers neurology, epidemiology, health economics, law/ethics, leadership, policy, creativity, and research methods.
Includes mentorship, networking, and opportunities for pilot projects.
Over 300 fellows from 65+ countries; strong alumni network.
Pilot Awards for Global Brain Health Leaders: Competitive small grants (~$25,000) for fellows’ innovative projects. These have leveraged tens of millions in additional funding and supported work in 45+ countries.
Research and Interventions:
Projects like PREVENT-Dementia (early detection and prevention; multi-center study with Trinity leadership).
Focus areas include caregiver burden, end-of-life care in dementia, social determinants of healthy aging (e.g., Latin America studies), sensory-cognitive links (hearing/vision), and emerging threats like climate change.
GBHI Projects: Larger faculty-led initiatives for training and scalable impact.
Advocacy and Knowledge Sharing:
Regional convenings, publications, media engagement, and policy influence (e.g., supporting national dementia plans).
Emphasis on creativity (e.g., arts in brain health) and global equity.
Trinity Connection and Integration
GBHI is housed within Trinity’s Institute of Neuroscience (TCIN), creating strong synergies with broader neuroscience research. It links closely to clinical psychiatry via leaders like Professors Lawlor and Leroi (St James’s Hospital) and aligns with Trinity’s strengths in geriatric psychiatry, cognitive neuroscience, and translational work. This builds on Trinity’s historical ties to psychiatric care (e.g., St Patrick’s) and complements TCIN’s focus on neuropsychiatry, neuroprotection, and brain health.Impact and Scale
Global network spanning 65+ countries.
Pilot projects have secured significant leveraged funding (tens of millions) and produced publications, media coverage, and real-world interventions.
Fellows and projects address prevention, care models, equity, and policy in diverse contexts.
High-profile support and events, including recent 10-year celebrations with Irish leaders and international figures.
Relevance to Broader Context (Psychiatry, Anxiety, TBI)
GBHI’s dementia/brain health focus overlaps with psychiatric conditions (e.g., late-life depression, anxiety in aging or neurodegenerative disease, caregiver mental health). Its life-course and equity lens could extend to prevention or mitigation of psychiatric sequelae after traumatic brain injury (TBI), inflammation/stress pathways, or cognitive/mental health resilience. The institute’s clinical ties (via St James’s and Trinity psychiatry) and interdisciplinary model make it relevant for translational work bridging neuroscience, psychiatry, and brain injury recovery.
Engagement and Opportunities
Fellowship applications: Annual cycles; details at gbhi.org/apply (Trinity or UCSF tracks).
Explore fellows, projects, and impact at gbhi.org.
Philanthropic support: As a major Atlantic-funded initiative, GBHI exemplifies how targeted giving advances brain health research and leadership. Bequests or donations to Trinity/TCIN can support related efforts (contact Trinity Development & Alumni).
GBHI represents a transformative, equity-driven model for addressing one of the 21st century’s biggest health challenges through leadership development and global collaboration. It strengthens Trinity’s position as a neuroscience and brain health hub.If you’d like deeper details on specific programs, fellows’ work, research projects (e.g., PREVENT), leadership transitions, or how it connects to bequests/TCIN/St Patrick’s psychiatry, let me know!
Explore PREVENT-Dementia study details
Learn about Atlantic Philanthropies history
Explore PREVENT-Dementia study details
Thought for 36s
PREVENT-Dementia (also styled as the PREVENT dementia programme) is a major multi-centre prospective cohort study focused on identifying midlife risk factors for dementia (particularly Alzheimer’s disease) and detecting the earliest preclinical indices of neurodegenerative disease—often decades before clinical symptoms appear. It targets midlife (roughly ages 40–59) as a critical “window of opportunity” for prevention and early intervention.
tcd.ie Aims and Rationale
The core goals are to:
Profile modifiable and non-modifiable midlife risk factors for later-life neurodegeneration.
Identify and describe the earliest brain changes (biomarkers) heralding dementia, especially Alzheimer’s.
Enable early detection, risk stratification, timely interventions (pharmacological and non-pharmacological), and development of novel treatments.
Advance understanding of how and when to intervene to reduce risk, support early diagnosis, and inform population-level prevention strategies.
It is one of the pioneering epidemiological initiatives emphasizing midlife intervention in neurodegenerative conditions, with a strong emphasis on deep phenotyping (detailed biological, imaging, cognitive, and lifestyle profiling) in cognitively healthy but at-risk individuals.
pmc.ncbi.nlm.nih.gov
History, Sites, and Collaborations
Initiated: 2014 as a single-site study in West London (led by Craig Ritchie and colleagues).
Expansion: Grew into a multi-centre study with sites in Edinburgh (2015), Oxford (2017), Cambridge (2017), and Dublin (2018).
Dublin/Trinity Site: Led by GBHI faculty members Professor Lorina Naci (Dublin co-lead; Trinity College Institute of Neuroscience and Global Brain Health Institute) and Professor Brian Lawlor (Founding Director, GBHI at Trinity; Conolly Norman Professor of Old Age Psychiatry). It operates in close collaboration with St James’s Hospital.
Broader Network: Involves researchers from Cambridge, Oxford, Edinburgh, Imperial College London, and INSERM Neuroscience (France). It serves as a research, training, and education platform for Atlantic Fellows in the Global Brain Health Institute (GBHI), with 15+ fellows involved.
Recent activity includes hosting the PREVENT General Assembly in Dublin, bringing together global experts. tcd.ie
Study Design and Methodology
PREVENT is a longitudinal prospective cohort study. Participants are cognitively healthy adults (screened via Addenbrooke’s Cognitive Examination-III) aged 40–59, often with elevated risk (e.g., parental family history of dementia or APOE ε4 genotype).Core Assessments (baseline and follow-ups):
Demographic, Lifestyle, and Psychological Data: Questionnaires on physical activity, diet, sleep, depression/anxiety (e.g., CES-D, STAI), resilience, stressful events, and traumatic brain injury history.
Cognitive Testing: Comprehensive battery including computerized tasks (COGNITO for attention/memory/visuospatial/language), virtual reality/spatial navigation tasks (e.g., Four Mountains Test, Virtual Supermarket Trolley for path integration), and global screening (ACE-III).
Neuroimaging: Multi-modal 3T MRI (structural: T1/T2/FLAIR/SWI; functional: resting-state and task-based fMRI; diffusion tensor imaging; arterial spin labelling; spectroscopy). Processed for volumetrics (e.g., hippocampus), cortical thickness, white matter hyperintensities, and more.
Biological Samples: Blood, saliva (including stress-response), urine; optional cerebrospinal fluid (CSF) via lumbar puncture. Genetic analysis (APOE genotyping and genome-wide).
Sub-Studies: Amyloid/tau PET imaging, virtual reality assessments, eye/hearing/dental evaluations, and others.
Recruitment: Via memory clinic relatives, dementia research registers (e.g., Join Dementia Research), word-of-mouth, and the study website (preventdementia.co.uk). Family/friends often invited. No geographic restrictions for some sites.Timeline: Baseline (2014–2020 across sites); follow-ups (e.g., ~2 years, then 5–8 years). Dublin site is in its later phases (first follow-ups concluding; plans for continued assessment).
pmc.ncbi.nlm.nih.gov Participants and Baseline Characteristics
Cohort Size: ~700 deeply phenotyped participants across sites (with substantial data from Dublin).
Demographics (baseline summary): Mean age ~51 years; ~62% female; highly educated (mean ~16.7 years); predominantly European ancestry.
Risk Profiling: Roughly equal split with/without parental dementia history. ~38% APOE ε4 carriers (including homozygotes). Categorized into low/medium/high risk groups. High prevalence of modifiable risks (e.g., overweight/obesity, physical inactivity, poor sleep, head injury history, hypertension).
Baseline data (published 2024 in Brain Communications) describe the cohort in detail and are openly shared via platforms like the Alzheimer’s Disease Data Initiative (ADDI). pmc.ncbi.nlm.nih.gov
Funding and Support
Core Funding: Alzheimer’s Society (UK) from 2014.
Dublin/Trinity: GBHI provided a €250,000 project grant in 2017 (to Naci and Lawlor) to initiate the site. Naci has since secured ~€1 million in additional competitive funding. In 2024, she received an HRB Individual Led Project award (€450,000) to extend the Dublin study into its eighth year (Trinity/St James’s).
Additional/Sub-Studies: UK Medical Research Council, US Alzheimer’s Association, industrial partners (~£2.9 million leveraged). The programme has enabled related work (e.g., sports head injury cohorts funded by English Football Association/FIFA).
Overall, PREVENT has attracted substantial investment and serves as a platform for further grants. tcd.ie
Key Findings and Outputs
Baseline Data (2024): Comprehensive description of the midlife cohort; subtle brain changes detectable in middle age among at-risk individuals. Data shared openly to accelerate research.
Recent Trinity-Led Insights (part of PREVENT): Engaging in physically, socially, and intellectually stimulating midlife activities (e.g., playing piano, foreign travel, socializing with friends) significantly boosts cognition—even in those with genetic or familial Alzheimer’s risk. This highlights modifiable lifestyle factors as powerful protective elements decades before typical onset.
Other outputs: Novel insights into early biomarkers (imaging, cognition, navigation/spatial tasks via VR), risk factor interactions, and preclinical Alzheimer’s changes. Over 40 publications; high-impact contributions to the field.
Broader Context: Aligns with global efforts (e.g., Lancet Commission on dementia prevention) emphasizing modifiable risks like traumatic brain injury (TBI), hypertension, and lifestyle. tcd.ie
Current Status and Future Directions
Ongoing: Longitudinal follow-ups continue; Dublin site actively building its dataset with preclinical biomarker assessments. Sub-studies (e.g., PET imaging, sensory assessments, athlete cohorts) are active or expanding.
Data Sharing: Baseline data available via ADDI and other platforms; imaging and code increasingly shared to support wider research.
Impact: Platform for GBHI Atlantic Fellows training; awareness-raising in Ireland; contributions to early-detection tools and prevention strategies. Expected to inform when and how to intervene (e.g., lifestyle or emerging therapies).
Challenges noted in publications include cohort demographics (highly educated, less ethnic diversity than general population) and the value of longer-term follow-up for symptomatic outcomes.
Relevance to Broader Brain Health Context
PREVENT complements GBHI’s focus on dementia prevention, equity, and life-course brain health. Its Trinity leadership (Naci in neuroscience/psychology; Lawlor in old age psychiatry) links directly to TCIN (imaging, cognition, neurodegeneration) and clinical psychiatry (St James’s). It addresses modifiable risks relevant to psychiatric conditions (e.g., depression, anxiety as risk factors) and post-TBI outcomes (TBI is a recognized dementia risk factor; lifestyle interventions may support resilience). The emphasis on early biomarkers and prevention aligns with translational neuroscience goals.For the latest details, visit preventdementia.co.uk or search recent publications (e.g., the 2024 Brain Communications baseline paper). Data requests are possible via the study’s steering processes.If you need specifics on a sub-study, particular findings, how it relates to bequests/TCIN/GBHI, or comparisons to other prevention trials, let me know!
Treasury Secretary Scott Bessent during a Senate Finance Committee hearing, June 3, 2026. Eric Lee—Bloomberg/Getty Images
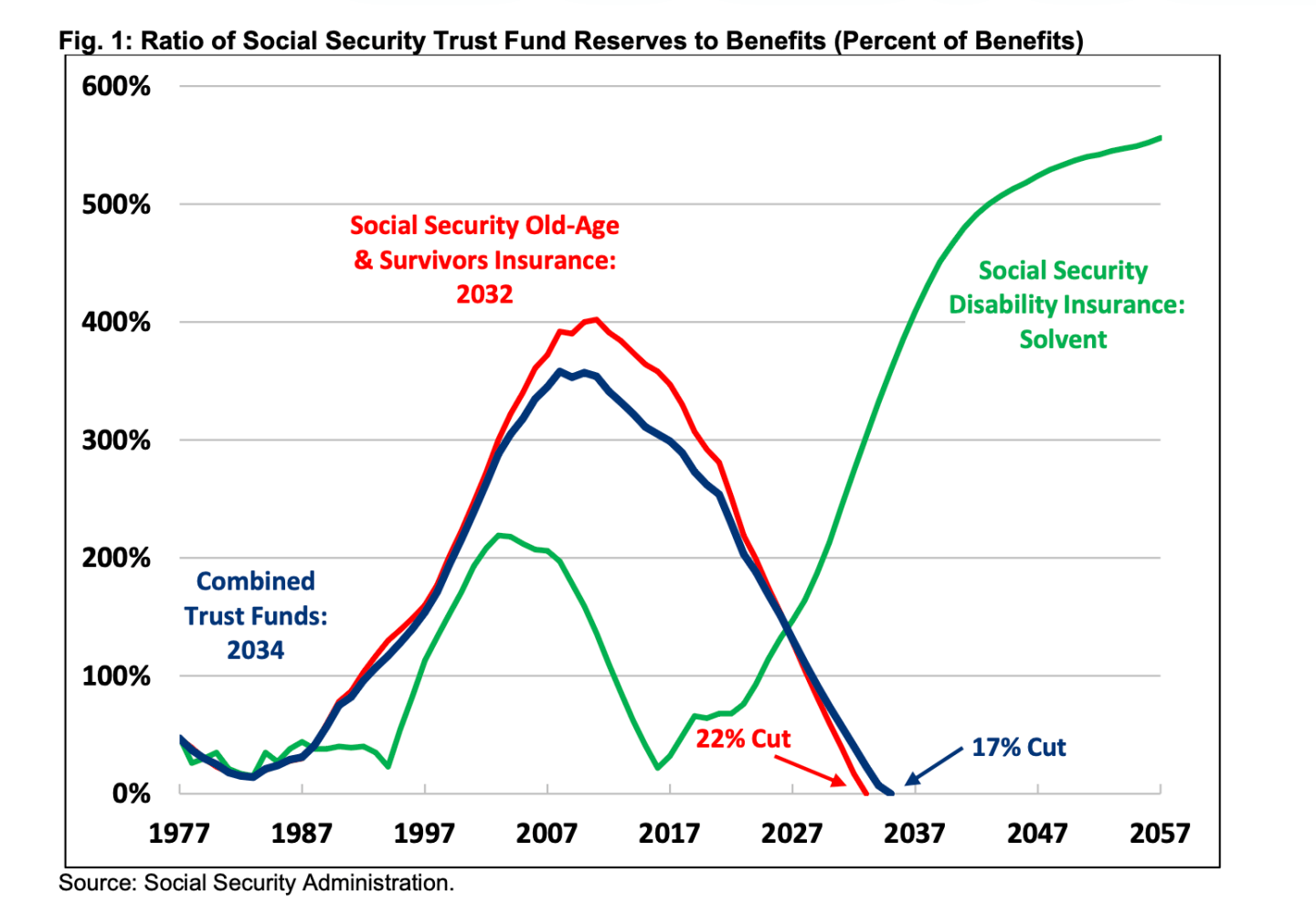
Social Security is hurtling toward a fiscal cliff that, if left unaddressed, will force an automatic 22% benefit cut for tens of millions of retirees, survivors, and their dependents in just six years.
That’s the stark warning from the release last week of the 2026 Social Security Trustees’ Report. A nonpartisan fiscal watchdog, the Committee for a Responsible Federal Budget (CRFB), found the program’s financial imbalance has reached its most severe point in nearly 50 years—and that inaction by lawmakers is making a bad situation measurably worse.
“Social Security is on a collision course toward insolvency,” the CRFB wrote in its analysis. “If policymakers fail to act, they will effectively be supporting a 22% benefit cut for all retirees, survivors, and their dependents in just six years.”The watchdog noted that the program hasn’t been so close to insolvency since 1983, when President Ronald Reagan and Speaker Tip O’Neill famously put partisanship aside to safeguard the program—until now.
The numbers are getting harder to ignore
The Old-Age and Survivors Insurance (OASI) Trust Fund—the primary fund that pays retirement benefits—is now projected to run dry in 2032, one year sooner than last year’s estimate. If disability insurance reserves are folded in, the theoretically combined trust funds exhaust in 2034, triggering a 17% across-the-board cut.
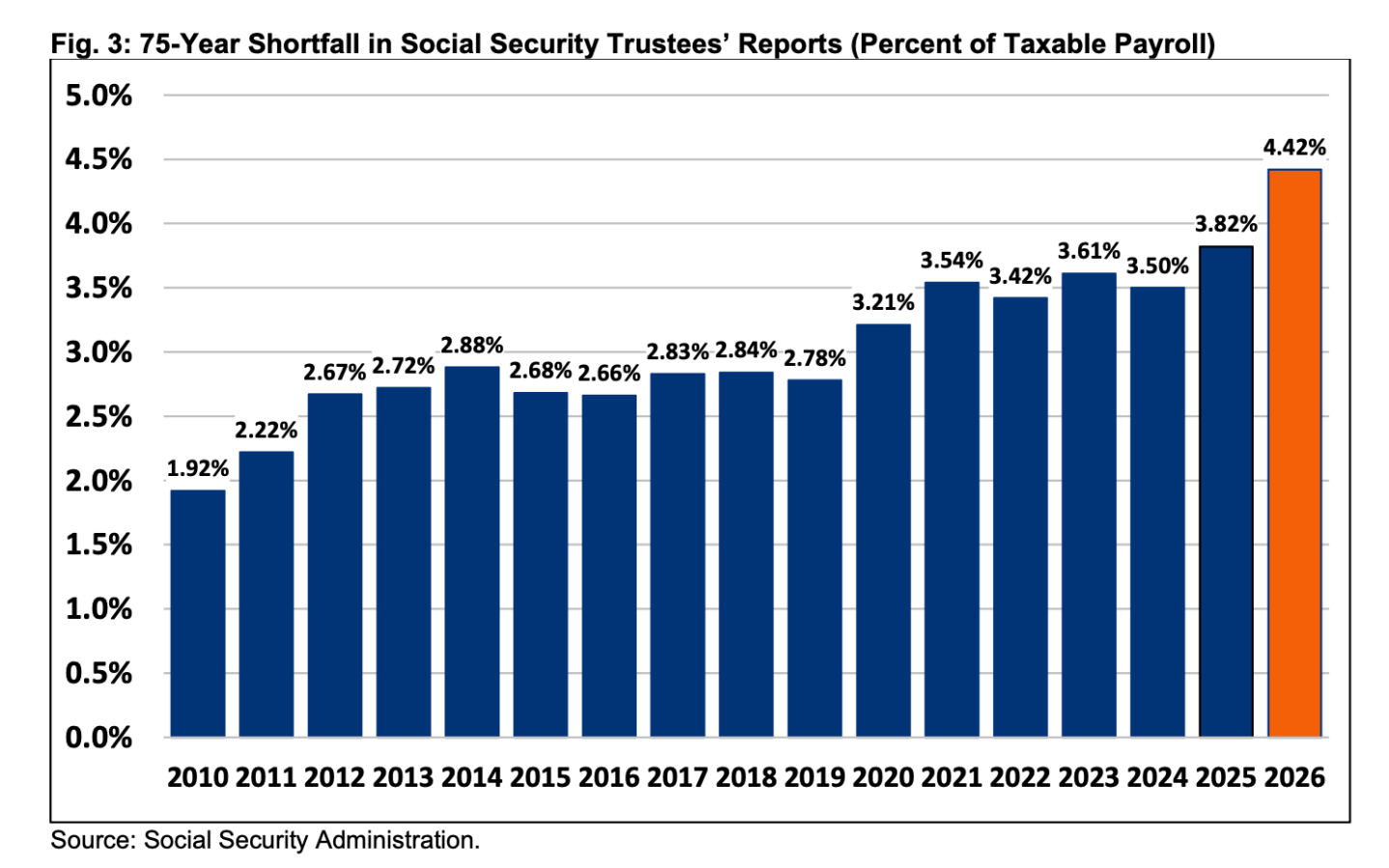
The 75-year actuarial shortfall has ballooned to 4.42% of taxable payroll, the largest since 1977, and equivalent to $31 trillion in present value—roughly the size of the entire U.S. economy.This is owing to lower fertility rates, a decline in immigration, and the unfunded spending in the One Big Beautiful Bill, and the gap has grown 16% in a single year, jumping from the 3.82% shortfall projected in last year’s report.
For context, the program’s deficit is now 2.3x as large as it was in 2010.
Over the next decade alone, Social Security will spend $3.8 trillion more than it collects. Annual deficits are projected to grow from 2.7% of taxable payroll today to 6.6% by 2100, driven by an aging population, growing benefit generosity, and revenues that simply won’t keep pace.
Treasury Secretary Scott Bessent has repeatedly insisted the administration will not touch benefits or raise taxes to address the shortfall.
“The senior citizen does not pay more taxes, and the senior citizen does not get less benefits,” Bessent told Congress earlier this month, framing faster economic growth—not structural reform—as the White House’s answer to a looming $31 trillion gap. His “3-3-3” framework—targeting 3% real GDP growth, 3% deficit-to-GDP, and 3 million additional barrels of daily energy production—has become the administration’s default response when pressed on specifics. Critics note the plan offers no direct mechanism to shore up the trust funds before the 2032 deadline.
Prominent economists and fiscal voices aren’t buying it. In a column published in Fortune, Johns Hopkins economist Steve Hanke and former U.S. Comptroller General David Walker (a former Social Security trustee himself) called for an emergency bipartisan fiscal commission—modeled on historical precedents—to generate binding, up-or-down reform votes in Congress, arguing the two programs together represent 36% of all federal spending and can no longer be deferred.
Writing in the New York Times, Harvard economist Jason Furman was equally blunt, having previously argued that reforms to Social Security and Medicare to eliminate their actuarial deficits must be a central pillar of any serious deficit-reduction framework, not an afterthought.
“I worked in the White House,” he wrote. “We never imagined the problem would get this bad.”
Meanwhile, Brookings researchers noted the troubling irony that the trustees’ report arrived more than two months late and without the sign-off of two public trustee positions that have sat vacant for over a decade—a sign, they wrote, that Washington is moving backward on reform.
A policy own goal
Deteriorating demographics explain most of the worsening outlook—but not all of it.
The trustees lowered their projected fertility rate from 1.9 to 1.75 children per woman, reflecting the ongoing decline in U.S. births, which alone accounts for 0.35 percentage points of the widened shortfall. Reduced immigration assumptions—the model now projects 1.2 million temporary or unlawfully present immigrants annually instead of 1.35 million—added another 0.21 percentage points.
But the third-largest contributor is a policy choice: the One Big Beautiful Bill Act, signed into law earlier this year, which cut taxes on Social Security benefits. The CRFB estimates the law reduced the actuarial balance by 0.16% of payroll, accounting for roughly a quarter of the year-over-year deterioration. The law also worsened Medicare’s Hospital Insurance trust fund shortfall by an additional 0.09% of payroll.
“A quarter of the increase was due to the enactment of the One Big Beautiful Bill Act, which reduced revenue from the income taxation of Social Security benefits,” the CRFB noted—a finding that puts the legislation in direct tension with the retirement security of the very voters it was designed to benefit.
The window is closing
Lawmakers still have options, but the menu is shrinking fast.
Acting today, Congress could restore long-term solvency through a 34% payroll tax increase (about 4.25 percentage points), a 25% cut in total benefits, or a 30% reduction for new beneficiaries. Wait until 2034, and those numbers jump: a 40% tax increase or a 29% benefit cut for everyone; at that point it would become mathematically impossible to close the gap by cutting benefits for new beneficiaries alone—even if those benefits were eliminated entirely.
Reforms that once seemed like silver bullets have lost their potency. Eliminating the payroll tax cap—currently set at $184,500 in wages—would now close only about half of the solvency gap, the CRFB found.
“Many options that would have once restored solvency are no longer available,” the watchdog wrote. “Continued inaction has the potential to take even more reforms off the table.”
A typical couple retiring in 2033 would face an $18,400 annual reduction in benefits if no action is taken before the trust fund runs out, which would be a life-altering income loss for households that have spent decades planning around those payments.
No state is spared
The impact won’t be evenly distributed, but it will be universal.
“No state will be spared from these cuts,” the CRFB warned, pointing to its own state-by-state analysis of what benefit reductions would mean on the ground.
The trustees themselves urged lawmakers to act, recommending they “address the projected trust fund shortfalls in a timely way in order to phase in necessary changes gradually and give workers and beneficiaries time to adjust.”
Solutions proposed by the CRFB’s Trust Fund Solutions Initiative include a “Six Figure Limit” on high earners’ benefits, a COLA (cost-of-living adjustment) cap, and a new Employer Compensation Tax—ideas designed to restore solvency while preserving retirement security and promoting economic growth.
“By failing to reform Social Security and Medicare,” the CRFB concluded, “policymakers are implicitly endorsing deep benefit and service cuts for most current and future beneficiaries.”
The clock, the report makes clear, is ticking—and it’s now just six years from midnight.
The Fortune 500 Innovation Forum will convene Fortune 500 executives, U.S. policy officials, top founders, and thought leaders to help define what’s next for the American economy, Nov. 16-17 in Detroit. Apply here.
A robot guided by an AI just performed surgery with near-perfect accuracy and no human intervention.
In a major step toward autonomous surgical systems, researchers at Johns Hopkins University have successfully trained an AI-guided robot to perform gall bladder removal on a dead pig with near-complete autonomy.
The dual-layer AI model—trained on 17 hours of human surgery footage—translated video input into verbal commands like “clip the second duct,” which were then converted into precise tool movements.
The robot completed all 17 surgical tasks across eight procedures with 100% task success, demonstrating real-time self-correction and only limited human intervention.
While full autonomy in live human surgeries remains years away, the milestone marks a significant advance in surgical robotics.
Experts emphasize that while the robot occasionally needed tool changes or adjusted missed grabs, its ability to detect and fix its own mistakes shows the growing reliability of AI-assisted procedures. With regulators expected to weigh in heavily before human applications, researchers plan to move next toward testing in live animals. The long-term goal? Safer, more precise surgeries that reduce complication rates and ease strain on surgical teams. source
Journal reference: Ji Woong (Brian) Kim. Science Robotics. 10 (4). SRT-H: A hierarchical framework for autonomous surgery via language-conditioned imitation learning