
It is being able to explain where those answers came from, which facts support them and what evidence could prove them wrong.
https://twitter.com/MGawdat/status/2086712948672577677/video/1
It is being able to explain where those answers came from, which facts support them and what evidence could prove them wrong.
https://twitter.com/MGawdat/status/2086712948672577677/video/1
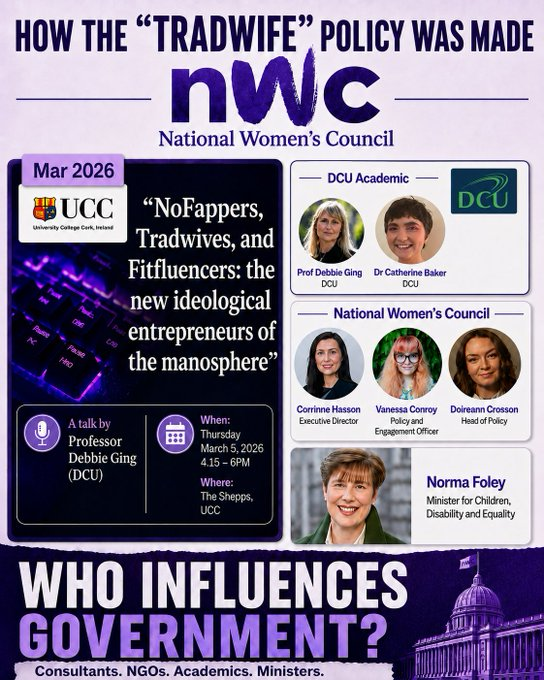
Govt funding for the National Women’s Council rose by 30% since the Family Care Referendum State Funding: 2024: €1.1million 2025: €1.43m (+30%!) Lets Recap:
The NWC wanted to remove Women & Mothers from the Constitution on Mother’s Day 2024. They backed the Yes/Yes proposal that suffered the largest referendum defeat in history. 73.93% rejection
In the aftermath of referendum, then CEO Orla O’Connor refused all media. (à la Dee Forbes) Regardless of all this, in 2025 the State awards the NWC a “unique role role in co-designing” the next National Women’s Strategy. The State gives them 30% boost in funding. They published a 36 page strategy document. Not one mention of the word “mother”.
The accompanying Action Plan runs to 52 pages. It does not use “mother” or “wife” once. It does however, include new policies around “tradwives” & the “manosphere”. Yet, the NWC provides no citation establishing the prevalence of either phenomenon in Ireland.
The most prominent Irish research into the “manosphere” and “tradwife” influencers is a DCU study, “Recommending Toxicity” This study used just ten fake accounts on ten blank smartphones as the basis for its entire research. It labelled as “toxic” content around “alpha masculinity” such as discipline, wealth and emotional stoicism. Read that last part again. *** *** *** Every part of this is absolutely ludicrous. Giving this amount of money, power & authority to a group of unelected, unintelligent activists cannot continue. Its time to de-fund the NGOs.
Here’s
@davidrkadler with a terrifying story about how tech oligarchs are trying to create their own start-up city-states, including in Latin America, and how far they are willing to go to protect these private fiefdoms. Honduras is Exhibit A.
https://twitter.com/NaomiAKlein/status/2086525217648808266/video/1
By
13/06/2020
Share on FacebookTweet on Twitter
This week on MIA Radio we turn our attention to electroconvulsive therapy (known as electroshock in the US). It’s fair to say that ECT remains a controversial subject with proponents and detractors regularly disagreeing on its safety and efficacy. The number of psychiatrists willing to administer ECT, particularly in the UK, is in decline but we are still using it to administer electric shocks to the brains of an estimated 2,000 people each year.
In this interview, we discuss a recent paper from the journal Ethical Human Psychology and Psychiatry. The title is ‘Electroconvulsive Therapy for Depression: A Review of the Quality of ECT versus Sham ECT Trials and Meta-Analyses’ and it is written by John Read, Irving Kirsch and Laura McGrath. On MIA we have previously written about the study and its findings.
We hear from two of the authors, Professor of Psychology John Read from the University of East London and Professor of Psychology Irving Kirsch from Harvard Medical School.
Richard P. Bentall: ECT is a classic failure of evidence-based medicine
By
26/07/2026
294
Share on FacebookTweet on Twitter
In January 24, 2023, Lindsay Clancy from Duxbury, Massachusetts took the lives of her three young children, Cora, 5, Dawson, 3, and eight-month-old Callan, and was charged with three counts of first-degree murder. She entered a not guilty plea at her arraignment on February 7. Her jury trial is starting on July 20 in Plymouth County, Massachusetts.
After Lindsay killed her children, she attempted suicide by taking a large quantity of various medications, cutting her wrists and neck, and jumping from a second-floor window into her backyard. She is now a paraplegic.

Clancy, who is 35 years old, had worked as a labor and delivery nurse at Massachusetts General Hospital in Boston for nine years before the birth of her third child, Callan, in May of 2022. Friends, family, and co-workers described her as a loving mother. Both her husband Patrick and Lindsay took family leave from their jobs for the next three months, and it was after he returned to work in late August that she became anxious, knowing that she too would soon have to return to work.
The prosecution appears to be intent on making a case that Clancy planned the attack, sending her husband out to run an errand and pick up dinner in order to buy herself time to kill their three children. Defense attorney Kevin J. Reddington will argue that she was suffering from postpartum mental illness and overmedication, and thus should be found not guilty by reason of insanity, or be acquitted because she was “involuntarily intoxicated” by the drugs.
As you can see by my bio, I took the life of my 11-year-old son, Ian, in 2004, three weeks after starting the SSRI antidepressant Paxil. I know how a psychiatric drug can take hold of your mind and push you into a psychotic state, and I hope that the jurors in this case ultimately will address this question: Is there any possibility that Lindsay Clancy, known by her friends and co-workers as a loving mother, would have killed her children if not for the intoxicating effects of the multiple psychiatric drugs she was on?
In January of this year, Patrick also filed a separate civil lawsuit against the providers of Lindsay’s psychiatric care. In his lawsuit, Patrick told of how after Callan was born, for the next three months both he and Lindsay were on family leave from their work, and they were both happy and well. In her lawsuit, Lindsay is described as hypomanic during these summer months, exercising very early in the morning, a routine that was described as impulsive.
On September 12, 2022, feeling stressed and anxious about returning to work, as her family leave was about to expire, she scheduled an appointment with a psychiatrist and was prescribed Zoloft as a remedy. Lindsay initially didn’t take the medication, as she thought it would interfere with her breastfeeding. However, in mid October, she decided to take the Zoloft.
Here is the record of her psychiatric treatment over the next three months, which was detailed in the civil lawsuit for medical malpractice that Lindsay filed:
• After she started taking the Zoloft, her psychiatrist increased her dose from 25 mg to 50 mg. Lindsay didn’t sleep for 48 hours, had racing thoughts, worsening anxiety, and felt “awful.”
• On October 20, Lindsay reported these adverse reactions to her psychiatrist. Her prescription for Zoloft was discontinued and she was prescribed Ativan and Benadryl for sleep.
• Lindsay’s insomnia persisted and she started having heart palpitations. Her mental health continued to deteriorate.
• On November 16, Lindsay’s insomnia had become so severe that she took herself to the emergency room at South Shore Hospital in Massachusetts. She reported insomnia, anxiety, and heart palpitations. A doctor prescribed Trazodone for sleep.
• On November 20, Patrick’s mother, a nurse at South Shore Hospital, contacted the South Shore Prenatal Behavioural Health Program seeking additional help for Lindsay because Trazodone was not effective at helping her sleep. A nurse practitioner reached out to Lindsay.
• On November 21, Lindsay told the nurse practitioner that she was “very frustrated and scared,” experiencing “extreme insomnia,” averaging only three to four hours of sleep a night, and was having racing thoughts. The nurse practitioner prescribed Prozac.
• After four days on Prozac, Lindsay reported that the medication made her insomnia worse. She informed the providers and Prozac was discontinued.
• On November 25, the nurse practitioner prescribed Ambien, Remeron and Klonopin.
• On November 28, Lindsay reported these symptoms to her providers, noting that she was still struggling, sleeping only three to four hours a night, and feeling disoriented and forgetful.
• On November 29, Lindsay started being treated by a different nurse practitioner. Lindsay reported that she was “anxious and frightened about what is happening” and that she blamed herself. The nurse practitioner prescribed Seroquel.
• After taking Seroquel, Lindsay developed suicidal ideation and began experiencing auditory hallucinations. The voice said “I will not be the same. I want to die.” She told Patrick, her parents and providers that her emotional state was “emotionless” and “like a zombie,” attributing this profound affective blunting to Seroquel.
• On December 2, Lindsay told the nurse practitioner that she had lost fifteen pounds, had no appetite, was experiencing panic attacks and confusion, and had a lack of attention over the past four days.
• On December 4, Lindsay was so frightened by the hallucinations that she called the New Bedford Suicide Hotline seeking help. She was told it was not an emergency because she didn’t have a specific plan about how she was going to kill herself.
• On December 5, Lindsay met virtually with an ASPIRE Crisis Support clinician seeking help. She was told that she didn’t meet the criteria for inpatient treatment because she didn’t have a suicide plan.
• On December 6, Patrick attended an appointment with Lindsay and the nurse practitioner. Patrick connected Lindsay’s suicidal thoughts to the Seroquel. He told the nurse practitioner that “Lindsay is ten thousand times worse since she has taken medication” and asked the nurse practitioner if they could “get Lindsay off medications and start from scratch to see what is going on.” He asked if there could be some mistake, like using wrong medications. The nurse practitioner acknowledged that it was possible. Despite this, the nurse practitioner continued to increase the Seroquel dosage towards 400 mg per day.
• On December 13, Lindsay was deeply depressed, wasn’t motivated to do anything, and still had suicidal ideation. She wanted “this to be all over.”
• On December 15, Patrick called the nurse practitioner’s office to report that “Lindsay has had a devastating week” and that today was the worst day for Lindsay. He explained that Lindsay felt debilitated, had no interest in anything, was exhausted, and could not get out of bed. She had horrible thoughts all day and auditory hallucinations all day, every day. The hallucinations were loud and continued all day saying, “I will never be the same,” “I will never be me again,” and “You are damaged. You will never be the same. The only option is to die.”
• Lindsay told Patrick, and her mother, that she had thoughts of harming her children. Lindsay was afraid of being locked in a hospital and having her children taken away.
• On December 20, Lindsay went to the Massachusetts General Hospital emergency room seeking help because her suicidal thoughts were escalating. They suggested either admission to McLean Hospital or the partial hospitalisation day program at Women & Infants Hospital in Providence, Rhode Island.
• On December 21, Lindsay admitted herself into the partial hospitalisation day program at Women & Infants Hospital in Providence, where she reported that she was numb to all emotion, feeling crazy, and depressed. She said that her “life is becoming a disaster,” that she was afraid and “messed up beyond repair.” Lindsay explained that she had lost 15 pounds in a month, wasn’t motivated to do anything, and that “it takes all of her effort in the world just to breathe.”
• The psychiatrist accepted Lindsay and Patrick’s belief that her symptoms were due to overmedication and recommended weaning her off Seroquel. The clinical team at Women & Infants concluded that Lindsay’s symptoms were pharmacologically induced so the day program was not appropriate for her.
• After Lindsay started reducing her Seroquel, her suicidal ideation “resurged.”
• On December 29, Lindsay told Patrick that “I can’t tough it out anymore. I need to go to McLean.”
• On December 30, Lindsay went to the emergency room at Massachusetts General Hospital, where she was told she should admit herself to a psychiatric hospital.
• On December 30, Lindsay admitted herself to McLean Hospital. Lindsay told staff that she was experiencing suicidal ideation, feeling detached, hopeless, and depressed, had no appetite or energy to perform daily activities, wasn’t motivated to do anything or enjoying anything anymore, had racing thoughts, wasn’t able to organize her thoughts, and was experiencing memory problems, anxiety, and insomnia.
• On January 3, 2023, Lindsay saw a doctor for the first time at McLean Hospital. The doctor advised Lindsay to stop Seroquel and the benzodiazepines and prescribed trazodone for sleep.
• On January 4, Lindsay asked if she could go home for Cora’s birthday. She was approved for discharge. The staff at McLean Hospital also suggested taking amitriptyline.
• On January 7, Lindsay was not herself at Cora’s birthday party. She smiled but did not converse. Lindsay avoided talking and could not make sense of what others were saying.
• Lindsay’s auditory hallucinations resumed a week after she was discharged from McLean Hospital.
• On January 10, Lindsay returned to the first psychiatrist and was prescribed Valium.
• On January 17, the psychiatrist prescribed amitriptyline at 10 mg per day.
• On January 20, because she was having such awful thoughts and was so numb and emotionless, Lindsay researched “What is a psychopath?” to see if she was one, and whether there was a cure.
• On January 23, Lindsay told her psychiatrist that she was a “little more anxious,” particularly in the morning. The psychiatrist increased the dosage of amitriptyline to 20 mg per day. That night, Lindsay didn’t sleep.
• On January 24, Lindsay was severely depressed with suicidal thoughts. She had suicidal hallucinations all day, nonstop. Later in the afternoon, a male voice began saying “You should harm the children.” When Patrick left to get takeout food for dinner, there was a loud, demanding, repetitious command from the male voice saying “This is your last chance. Kill the children so you can kill yourself.” Lindsay felt an overwhelming, irresistible compulsion to comply, entering a “dream-like state” where her physical actions felt utterly disconnected from her conscious volition and strangled her three children, then attempted suicide.
That is her record of psychiatric care. It tells of how Lindsay Clancy steadily worsened while under the influence of psychiatric drugs, and how at each step she desperately sought medical help. This is the record that would support an acquittal of involuntary intoxication, which I believe would be the just verdict in this tragic case.
***
Mad in Ireland hosts blogs by a diverse group of writers. These posts are designed to serve as a public forum for a discussion—broadly speaking—of psychiatry and its treatments. The opinions expressed are the writers’ own. This post first appeared on Mad in America
SHARE
Previous articleChallenging the medical model of mental health: A call for humane, evidence-based services

File photo of members of Boko Haram terrorist organization. Photo Credit: Tasnim News Agency
FacebookTwitterEmailFlipboardMastodonLinkedInShare
Video Muted
Boko Haram’s first female suicide bomber killed herself and a Nigerian Soldier in 2014 at a barracks in Gombe State. Since then, Boko Haram has deployed more female suicide bombers than any other terror group in history, conducting a form of asymmetric warfare that analysts say has a deep psychological impact on communities.
“Notably, many of these attacks involve coercion, with abducted women and girls forced into suicide missions, often without their full awareness,” analyst Usman Anwar wrote in The Diplomatic Insight. “This represents a significant departure from earlier cases where ideological commitment or personal motivation played a central role.”
“By weaponizing women and young girls, traditionally viewed as non-combatants, Boko Haram disrupts cultural expectations in ways that reverberate within affected communities,” Victoria Maldonado wrote for Georgetown University’s Security Studies Review. “This tactic undermines the perception of safety within traditionally feminine spaces, such as homes, schools, and markets, turning places of refuge into sites of potential violence.”
Historically, men have dominated the planning and execution of terrorist attacks. By deploying female bombers, terror groups exploit social norms that cause security forces to view women with less suspicion. Terror groups take advantage of this by directing women to hide explosives in their robes or beneath their hijabs.
“This trend not only challenges security frameworks but also raises profound ethical dilemmas about agency and coercion in violent extremism,” Maldonado wrote. “The incorporation of women into terrorist activities complicates the narrative of victim and perpetrator.”
While some women commit suicide bombings voluntarily, many are forced to do so against their will, she added. Sexual and mental abuse are often used to break down women psychologically and destroy their social standing so that suicide becomes an avenue to escape the shame.
Analysts are divided on the significance of the recent surge in female suicide bombers. Some see it as the last option of terror groups employing “shock value” as they face significant losses on the battlefield. Others see suicide bombings as an indicator of a group’s strength, such as ISWAP’s growing presence in the Lake Chad Basin.
The threat of female suicide bombers puts security forces into an untenable position: If they allow the bomber to slip through undetected, people die. If they kill a suspected bomber, they create a propaganda incident for the group that sent her, according to analysts.
Female bombers can also be used to shame men reluctant to commit to such actions, according to Anwar.
“This aligns with the concept of the ‘propaganda of the deed,’ where the symbolic impact of an attack is as important as its physical consequences,” Anwar wrote.
Security experts may be able to use advances in surveillance and artificial intelligence to detect female suicide bombers early, reducing the risk to civilians and avoiding the propaganda victory terrorists seek, Anwar added.
“Militant groups are likely to adapt by exploiting new vulnerabilities, particularly those rooted in social and cultural norms,” he wrote. “The continued evolution of this phenomenon underscores the adaptive nature of non-state actors in asymmetric warfare.”

The Africa Defense Forum (ADF) magazine is a security affairs journal that focuses on all issues affecting peace, stability, and good governance in Africa. ADF is published by the U.S. Africa Command.
Katharina Kroll in Iceland
August 7, 2026
Security concerns, control over fishing rights and rising living costs are shaping Iceland’s debate over whether to restart talks on joining the European Union.
The white church stands alone in the Icelandic countryside. Wind sweeps across the Hvalfjord. Kristjan Ingolfsson, a retired bishop, lives here beside Hallgrimskirkja church in Saubaer, surrounded by silence and vast open landscapes.
But far from this quiet corner of western Iceland, the debate over Europe is heating up. At the end of August, voters will decide whether to reopen accession talks with the European Union. The referendum is not about joining the EU immediately, but about restarting negotiations that were suspended more than a decade ago.
“[Icelandic] people are a bit different to the mainland folks, who always have to think about borders. We have no border, just the sea all around,” Kristjan Ingolfsson says.
“That gives a specific feeling of freedom. And I believe that’s also part of the whole discussion, that people want to be free.”
Whether campaigning for or against closer ties with Brussels, many Icelanders frame the debate around the same ideas: freedom, independence, and sovereignty.
At the headquarters of the pro-European group in the capital, Reykjavik, supporters are celebrating the official launch of the campaign. The small office is packed, with volunteers spilling onto the pavement in the afternoon sun. Young people mingle with pensioners. A DJ provides music while beer and soft drinks are kept chilled in ice buckets.
At the center of it all is Snaeros Sindradottir, executive director of the ‘Yes’ campaign. The 34-year-old mother normally runs an art gallery, but that work is now on hold. Instead, she spends her days campaigning for a closer relationship with Europe.

The referendum is taking place at a time of growing geopolitical uncertainty. US President Donald Trump‘s threats toward neighboring Greenland have become part of Iceland’s debate over Europe, says Snaeros Sindradottir.
“And it’s not a very comforting fact that Trump has mispronounced Greenland as Iceland on several occasions.”
Iceland, with its population of about 400,000, has no standing army. Protection is provided through NATO, of which Iceland is a founding member. The country also has a bilateral defense agreement with Washington. During the Cold War, the US maintained an important military base near Reykjavik, although its permanent troop presence ended in 2006.
“I think security would definitely be increased if we enter the EU,” says Snaeros Sindradottir.
“Given the situation in the United States, it would be wiser to lean [on] our true allies and friends in Europe.”
Iceland is already closely tied to Europe. The country belongs to the European Economic Area (EEA), allowing free movement of goods, services, capital and people between Iceland and most EU countries, even though the island nation is not an EU member. It is also part of the passport-free Schengen zone.
https://www.dw.com/webapi/iframes/widget/en/76105179
Pawel Bartoszek, chairman of parliament’s foreign affairs committee, points to Iceland’s small and relatively volatile currency.
“It has cost us much higher inflation and interest rates compared to continental Europe,” he says.
Bartoszek argues that joining the euro in the future could lower borrowing costs for households and businesses. Mortgage rates of 8 to 9% are common in Iceland, while borrowers elsewhere in Europe often pay roughly half as much.
In downtown Reykjavik, campaigners from the anti-EU movement are making the opposite case. They have set up a small table where they hand out leaflets and “No” campaign badges. Haraldur Olafsson, a physics professor, currently spends up to 12 hours a day campaigning against membership.
“We are basically here to explain to the people that being members of the European Union is a huge step away from democracy.”
“We are giving power to someone else who will make rules that we cannot control,” he adds.
For years, Haraldur Olafsson has campaigned against joining the EU. He is the president of the Heimssyn organization, which belongs to the ‘No’ camp.

The ‘No’ campaign’s stand is quiet today. Tourists crowd the square opposite parliament, every now and then Olafsson is approached by acquaintances. This is Iceland. People know each other here.
“I do not know anybody in Iceland who fears either the Russians or the Americans,” Haraldur Olafsson says.
“Really, I don’t think these international matters matter a lot when it comes to local politics. The only threat comes from the European Union. The European Union is the only big power in the world that wants to govern Iceland, that wants to set the laws in Iceland and wants to pass judgment.”
Supporters of EU membership reject this argument, saying that as an EU member Iceland would participate in decision-making rather than simply follow rules set elsewhere.
https://www.dw.com/webapi/iframes/widget/en/76806093
Iceland’s thriving fishing industry is one of the foundations of the country’s prosperity. That is why the debate over possible EU membership has become highly emotional, with both sides arguing over whether the European Union would gain control over Iceland’s valuable marine resources.
“The European Union has nothing to say about the natural resources in Iceland — the sea, the fish,” Haraldur Olafsson says.
“The European Union doesn’t have the final word on energy, which is a very important natural resource for Iceland.”
“The economy of Iceland is very different from the economy of Europe. The main disadvantage is that the EU would take over the administration of [our] natural resources,” he argues.

Haraldur Olafsson heads down to Reykjavik’s harbor. Here he meets former fisherman Agust Österby, who is standing on his wooden boat, fixing an old window frame. Österby first went to sea with his father when he was six years old. Today, he restores wooden boats.
Icelanders, he says, are stubborn and independent by nature.
“It is somehow in our genes to deal with [things] ourselves — to deal with life, the sea and the weather.”
He adds: “We will never give our freedom to the European Union. We know exactly how to do things in Iceland. We don’t need help from abroad.”
The former fisherman says he does not think Icelanders feel threatened by anyone — not even Donald Trump.
The belief that Iceland can simply keep a low profile and avoid international pressure is something political scientist Audunn Arnorsson disagrees with. He fears the strategy “might backfire.”
If Iceland were ever to face pressure similar to that experienced by Greenland from its “big brother in the West,” having the possibility of EU accession could prove valuable, including access to the bloc’s common customs protection.
Iceland had already begun accession negotiations once before, in 2010, following the banking and economic crisis. They were later suspended after a change in government and never resumed. Audunn Arnorsson argues that holding a referendum became the only way to break the political deadlock over whether Iceland should reopen negotiations.
Members of Iceland’s parliament are also divided over whether the country should resume accession talks with the European Union. The debate cuts across traditional party lines.
Gudrun Hafsteinsdottir, leader of the opposition Independence Party, believes that a small nation like Iceland may have a bigger voice outside the European Union than inside.
“In the European Parliament, we would have approximately six seats out of 726. We are afraid that we will just disappear in this mass that the European Union is.”
Smaller EU member states such as Malta, Luxembourg and Cyprus also hold the minimum allocation of six seats in the European Parliament.

For Gudrun Hafsteinsdottir, joining the EU is not the solution for strengthening Iceland’s security.
“Our strength lies in NATO and our bilateral agreement with the United States of America. And we have not had any discussion from [the] American side that they want to change that agreement that we have had here in Iceland for decades.”
But something else concerns the opposition leader deeply: the divisions the debate has created within families and friendships.
“We are building a wound that won’t heal [for] years. We can’t survive in this harsh country if we don’t have solidarity between us, so that we can fight Mother Nature.“
Opinion polls predict a tight race, with support for and opposition to closer EU integration running neck and neck. Both camps are now fighting for the same group: the many undecided voters who are likely to determine the result on August 29.
A ‘yes’ vote would not mean EU membership. It would only open accession talks — with a second referendum required before Iceland could ultimately join the bloc.
But former bishop Kristjan Ingolfsson is confident: “No matter how it turns out — we will remain one people and [it will] not build walls between us.”
 Mad in the UK
Mad in the UK
.){kind=link}
{kind=link}