
A Look at the New Executive Order and the Intersection of Homelessness and Mental Illness
Authors: Heather Saunders and Robin Rudowitz
Published: Aug 15, 2025 Print
Email Copy Link
President Trump recently signed an executive order on homelessness, mental health, and substance use that leverages federal funding priorities and other administrative tools to encourage states to ban public drug use, remove unhoused people from public spaces, and broaden civil commitment laws to permit involuntary psychiatric civil commitments in more circumstances. It also instructs the Department of Housing and Urban Development (HUD) to end funding for programs that use the “Housing First” approach–which provides immediate housing without preconditions such as sobriety or mandatory mental health treatment—and instead to fund programs that require individuals to participate in treatment prior to receiving housing assistance. The executive order comes about one year after the 2024 Supreme Court decision (Grants Pass v. Johnson), which makes it easier for law enforcement to ticket, fine, or arrest people sleeping on public property. Approximately 220 local governments have since passed enforcement measures targeting homelessness.
Weeks after signing the executive order, President Trump announced plans to deploy the National Guard and assume control of D.C. police to clear homeless encampments in the city and address crime. While he did not specify where unhoused people would be relocated, he posted that they would be given “places to stay, but far from the capital.” These actions align with his campaign statements advocating for relocation of unhoused individuals to “tent cities” and expanding involuntary psychiatric commitments, including his campaign remarks that people with serious mental illnesses (SMI) should be brought “back to mental institutions, where they belong.”
Taken together, these policies represent a departure from decades of court-backed deinstitutionalization, which emphasized voluntary, community-based care in less restrictive settings. They also work together by pairing easier state expansion of law- enforcement authority related to homelessness with federal incentives to encourage states to broaden civil commitment laws and psychiatric institutional care.
This brief describes the new executive order, examines the intersection of homelessness and mental illness, reviews the history of the deinstitutionalization movement, and discusses specialized treatment services for people with SMI.
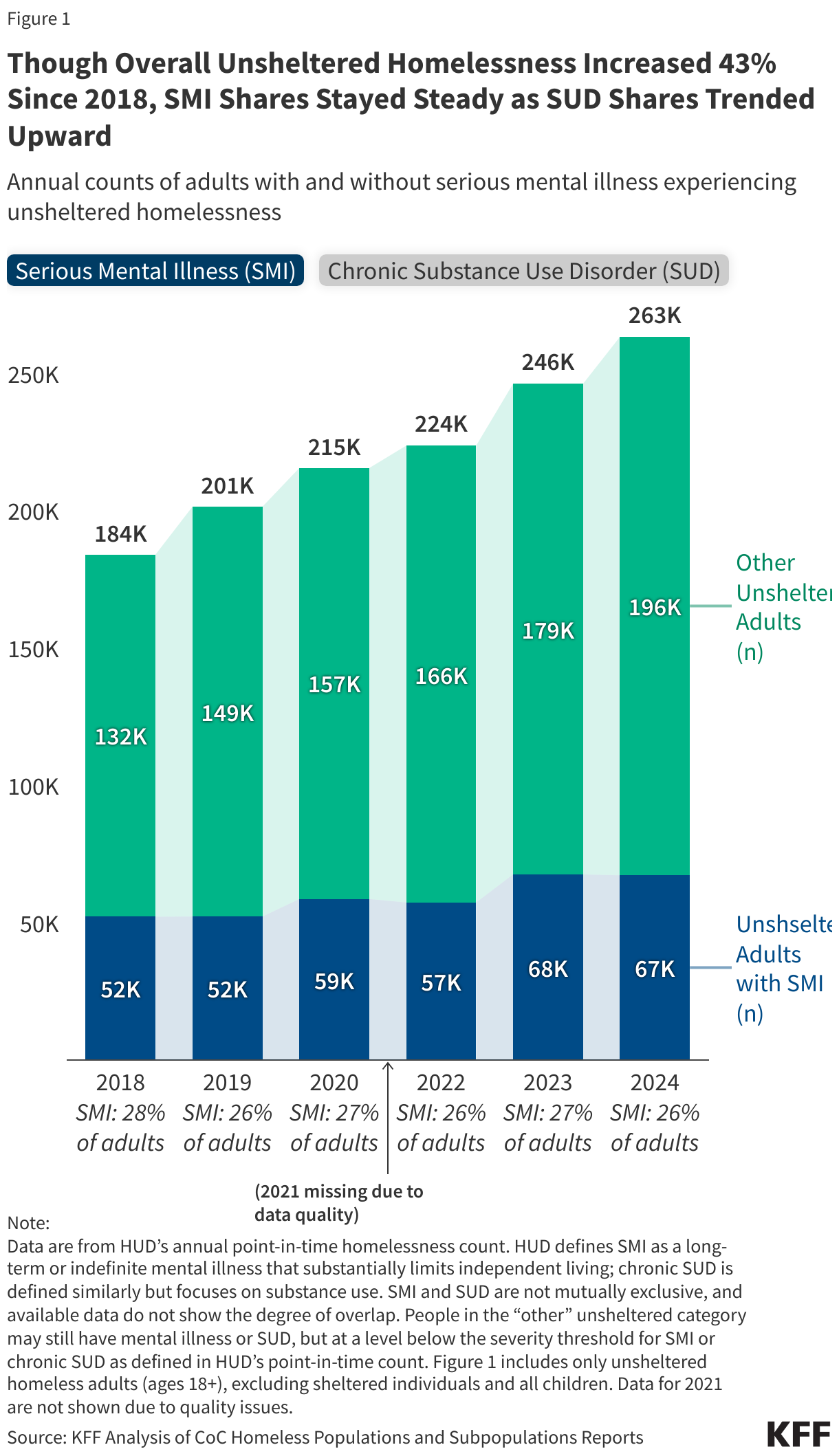
In 2024, about one-quarter (26%) of adults experiencing unsheltered homelessness had a serious mental illness and a similar share had a chronic substance use disorder—both higher than the general population. HUD’s annual point-in-time count defines SMI as a mental illness that substantially limits independent living and is expected to be of long-lasting or indefinite duration. Specifically, 26% (67,000 of 263,000) of adults experiencing unsheltered homelessness met HUD’s SMI definition (Figure 1), compared to about 5-6% of adults overall according to the National Survey of Drug Use and Health (NSDUH). A similar share—about 26%—were identified as having a chronic substance use disorder (SUD) according to HUD’s definition in the point-in-time count, compared to about 3% of adults in the general population who met NSDUH criteria for severe SUD. SMI and SUD often co-occur—about one-quarter of people with SMI also has an SUD—but HUD’s publicly available data do not report the overlap of these conditions. This analysis focuses on unsheltered adults to more closely align with the population described in the executive order; unsheltered adults account for about 40% of all adults experiencing homelessness, with the remainder in sheltered settings (emergency shelters and transitional housing). The shares with SMI or chronic SUD are higher among unsheltered adults than sheltered adults (SMI: 26% vs. 20%; SUD: 26% vs. 12%). Data are not shown for 2021 due to data reliability issues. SMI is a category encompassing more severe mental illnesses, not a single diagnosis, and conditions classified as SMI vary in presentation and severity within and across populations. Prevalence estimates also differ across studies because mental illness and homelessness can be defined and measured differently.
The number of adults experiencing unsheltered homelessness increased by more than 40% since 2018, while the share with serious mental illness has remained relatively stable and the share with chronic SUD trended upward. From 2018 to 2024, the number of adults experiencing unsheltered homelessness grew by 43%, while the share of those with SMI edged down from 28% to 26% and the share chronic SUD increased somewhat from 22% to 26%, potentially reflecting the ongoing opioid crisis. Because these shares changed little overall, most of the increase occurred among adults not identified as having SMI or chronic SUD (though the overlap is unknown). This pattern suggests that broader factors, such as housing affordability are also contributing to increases in unsheltered homelessness.
Note:
Data are from HUD’s annual point-in-time homelessness count. HUD defines SMI as a long-term or indefinite mental illness that substantially limits independent living; chronic SUD is defined similarly but focuses on substance use. SMI and SUD are not mutually exclusive, and available data do not show the degree of overlap. People in the “other” unsheltered category may still have mental illness or SUD, but at a level below the severity threshold for SMI or chronic SUD as defined in HUD’s point-in-time count. Figure 1 includes only unsheltered homeless adults (ages 18+), excluding sheltered individuals and all children. Data for 2021 are not shown due to quality issues.
Source: KFF Analysis of CoC Homeless Populations and Subpopulations ReportsGet the dataDownload PNG
.png)
President Trump’s executive order seeks to widen the use of involuntary civil commitments for adults experiencing homelessness and serious mental illness, shifting away from deinstitutionalization efforts. Civil commitment is a legal process in which a court orders an individual with a SMI into involuntary treatment–either in a hospital or through supervised outpatient care (“assisted outpatient treatment“)—for a defined period. Each state sets its own civil commitment rules, but these must comply with federal laws and constitutional rights. Typically, civil commitment is limited to cases where an individual’s mental illness creates a significant risk of harm to themselves or others. To expand civil commitments, the executive order directs the Attorney General and HHS Secretary to pursue reversals of court decisions that currently limit the use of civil commitments, and to provide guidance to states to make civil commitment standards more flexible, including for involuntary inpatient and outpatient treatments. It also instructs several federal officials—including the Attorney General and Secretaries of HHS and HUD—to review discretionary grant programs and prioritize funding for states that ban public drug use and urban camping and use civil commitment or other legal actions to move unhoused people into treatment. Additionally, the executive order directs agencies to collect data from homelessness assistance programs and allow sharing with other agencies, such as law enforcement.
Before deinstitutionalization, people with serious mental illnesses were often housed in long-term psychiatric institutions, but advances in treatment, growing public concern about poor institutional conditions, and civil rights litigation shifted care to community-based settings. Approval of the first antipsychotic drug in the 1950s and growing public awareness of the poor conditions in mental institutions sparked the deinstitutionalization movement—which shifted mental care away from long-term institutional care toward community-based treatment. The 1963 Community Mental Health Act introduced federal funding to transition care to community mental health centers (CMHCs), which were intended to provide five core services: inpatient, outpatient, emergency, partial hospitalization, and consultation/education. Medicaid was passed in 1965, which further reinforced the deinstitutionalization transition by reimbursing community-based mental health services while prohibiting payment for care in Institutions for Mental Diseases (IMDs). CMHC development fell short of the original vision, with fewer than half of planned centers built and many centers focused less than expected on people with severe mental illnesses that had previously been institutionalized in state facilities. President Carter sought to close some gaps through passage of the Mental Health Systems Act (MHSA), which planed to expand services for those with chronic SMI and to tighten accountability through performance-based contracts and monitoring. However, President Reagan reversed course by repealing the MHSA, converting federal funds into state block grants, cutting funding by 25%, and barring the use of grant funds for inpatient psychiatric care—a restriction that persists today. Philanthropic initiatives helped respond to gaps in health care through community-based health responses to homelessness. Meanwhile, federal civil rights laws and litigation from the 1990s and earlier affirmed the right of people with SMI to receive treatment in the least restrictive setting, reinforcing deinstitutionalization.
As mental health services shifted toward outpatient care, the availability of psychiatric inpatient beds declined from 237 residents in beds per 100,000 in 1970 to 37 per 100,000 in 2020. Over time, psychiatric inpatient care has shifted in both populations served and facility characteristics. Facilities once housed people with developmental and intellectual delays, as well as dementia, but after the 1970s, they primarily served individuals with mental illness. Long-term stays, once common, are now less common, and inpatient care has expanded to include psychiatric beds in general hospitals and non-state residential facilities, most of which focus on shorter-term stays. It isn’t clear to what extent this historical reduction in psychiatric beds directly explains current homelessness. In 2023, the demand for inpatient and residential psychiatric beds exceeded the bed supply by over 3,500 beds. This count does not include instances where those experiencing psychiatric emergencies left in the emergency department before being seen or gaining access to a bed. When psychiatric beds are unavailable, admitted patients may be “boarded” in emergency departments, a practice most common among patients with psychotic or bipolar disorders and those who are involuntarily committed.
see KFF for graphs and tables
Over time, community-based treatment has expanded due to deinstitutionalization, but specialized outpatient services remain limited, and overall shortages persist. Evidence-based treatment designed specifically for people with the most mental health needs have shown effectiveness in reducing acute care use, shortening hospital stays, and supporting people with SMI experiencing homelessness. For example, Assertive Community Treatment (ACT) provides 24-hour support through small, multidisciplinary teams that individualize care, intensifying support services during symptom flare-up and reducing it when symptoms stabilize. ACT is sometimes used in conjunction with Assisted Outpatient Treatment, a form of civil commitment requiring adherence to medication or outpatient treatment. Other evidence based practices include Permanent Supportive Housing and First Episode Psychosis (FEP) programs; however, these programs are limited, vary by state and region, and many struggle with workforce shortages.
Decreases in federal spending may leave states with even fewer resources to put toward treatment options for those with serious mental illnesses, including those at risk of homelessness. Although the executive order promotes expanding civil commitment and institutional care for unhoused individuals with SMI, it does not provide new federal funding to support these efforts. Federal rules generally prohibit Medicaid and community mental health block grant dollars from financing care in psychiatric facilities with more than 16 beds (known as Institutions for Mental Disease, or IMDs), except under specific circumstances or through Medicaid IMD waivers. Additionally, the Trump administration proposed significant cuts to behavioral health and housing programs, including a reduction of over $1 billion to SAMHSA–which funds behavioral health initiatives such as block grants— and a proposed 50% cut to HUD, the federal agency that manages housing assistance funds. While the final scale of these cuts is uncertain as congressional committees currently deliberate, substantial reductions to Medicaid spending have already been enacted through the recent reconciliation package, potentially affecting both Medicaid coverage and access to behavioral health services. Reductions in federal funding and coverage are likely to exacerbate existing capacity constraints to inpatient and outpatient behavioral health services.
More On












{kind=link}